

Is it time to get rid of homework? Mental health experts weigh in.
It's no secret that kids hate homework. And as students grapple with an ongoing pandemic that has had a wide range of mental health impacts, is it time schools start listening to their pleas about workloads?
Some teachers are turning to social media to take a stand against homework.
Tiktok user @misguided.teacher says he doesn't assign it because the "whole premise of homework is flawed."
For starters, he says, he can't grade work on "even playing fields" when students' home environments can be vastly different.
"Even students who go home to a peaceful house, do they really want to spend their time on busy work? Because typically that's what a lot of homework is, it's busy work," he says in the video that has garnered 1.6 million likes. "You only get one year to be 7, you only got one year to be 10, you only get one year to be 16, 18."
Mental health experts agree heavy workloads have the potential do more harm than good for students, especially when taking into account the impacts of the pandemic. But they also say the answer may not be to eliminate homework altogether.
Emmy Kang, mental health counselor at Humantold , says studies have shown heavy workloads can be "detrimental" for students and cause a "big impact on their mental, physical and emotional health."
"More than half of students say that homework is their primary source of stress, and we know what stress can do on our bodies," she says, adding that staying up late to finish assignments also leads to disrupted sleep and exhaustion.
Cynthia Catchings, a licensed clinical social worker and therapist at Talkspace , says heavy workloads can also cause serious mental health problems in the long run, like anxiety and depression.
And for all the distress homework can cause, it's not as useful as many may think, says Dr. Nicholas Kardaras, a psychologist and CEO of Omega Recovery treatment center.
"The research shows that there's really limited benefit of homework for elementary age students, that really the school work should be contained in the classroom," he says.
For older students, Kang says, homework benefits plateau at about two hours per night.
"Most students, especially at these high achieving schools, they're doing a minimum of three hours, and it's taking away time from their friends, from their families, their extracurricular activities. And these are all very important things for a person's mental and emotional health."
Catchings, who also taught third to 12th graders for 12 years, says she's seen the positive effects of a no-homework policy while working with students abroad.
"Not having homework was something that I always admired from the French students (and) the French schools, because that was helping the students to really have the time off and really disconnect from school," she says.
The answer may not be to eliminate homework completely but to be more mindful of the type of work students take home, suggests Kang, who was a high school teacher for 10 years.
"I don't think (we) should scrap homework; I think we should scrap meaningless, purposeless busy work-type homework. That's something that needs to be scrapped entirely," she says, encouraging teachers to be thoughtful and consider the amount of time it would take for students to complete assignments.
The pandemic made the conversation around homework more crucial
Mindfulness surrounding homework is especially important in the context of the past two years. Many students will be struggling with mental health issues that were brought on or worsened by the pandemic , making heavy workloads even harder to balance.
"COVID was just a disaster in terms of the lack of structure. Everything just deteriorated," Kardaras says, pointing to an increase in cognitive issues and decrease in attention spans among students. "School acts as an anchor for a lot of children, as a stabilizing force, and that disappeared."
But even if students transition back to the structure of in-person classes, Kardaras suspects students may still struggle after two school years of shifted schedules and disrupted sleeping habits.
"We've seen adults struggling to go back to in-person work environments from remote work environments. That effect is amplified with children because children have less resources to be able to cope with those transitions than adults do," he explains.
'Get organized' ahead of back-to-school
In order to make the transition back to in-person school easier, Kang encourages students to "get good sleep, exercise regularly (and) eat a healthy diet."
To help manage workloads, she suggests students "get organized."
"There's so much mental clutter up there when you're disorganized. ... Sitting down and planning out their study schedules can really help manage their time," she says.
Breaking up assignments can also make things easier to tackle.
"I know that heavy workloads can be stressful, but if you sit down and you break down that studying into smaller chunks, they're much more manageable."
If workloads are still too much, Kang encourages students to advocate for themselves.
"They should tell their teachers when a homework assignment just took too much time or if it was too difficult for them to do on their own," she says. "It's good to speak up and ask those questions. Respectfully, of course, because these are your teachers. But still, I think sometimes teachers themselves need this feedback from their students."
More: Some teachers let their students sleep in class. Here's what mental health experts say.
More: Some parents are slipping young kids in for the COVID-19 vaccine, but doctors discourage the move as 'risky'
Along with Stanford news and stories, show me:
- Student information
- Faculty/Staff information
We want to provide announcements, events, leadership messages and resources that are relevant to you. Your selection is stored in a browser cookie which you can remove at any time using “Clear all personalization” below.

Education scholar Denise Pope has found that too much homework has negative effects on student well-being and behavioral engagement. (Image credit: L.A. Cicero)
A Stanford researcher found that too much homework can negatively affect kids, especially their lives away from school, where family, friends and activities matter.
“Our findings on the effects of homework challenge the traditional assumption that homework is inherently good,” wrote Denise Pope , a senior lecturer at the Stanford Graduate School of Education and a co-author of a study published in the Journal of Experimental Education .
The researchers used survey data to examine perceptions about homework, student well-being and behavioral engagement in a sample of 4,317 students from 10 high-performing high schools in upper-middle-class California communities. Along with the survey data, Pope and her colleagues used open-ended answers to explore the students’ views on homework.
Median household income exceeded $90,000 in these communities, and 93 percent of the students went on to college, either two-year or four-year.
Students in these schools average about 3.1 hours of homework each night.
“The findings address how current homework practices in privileged, high-performing schools sustain students’ advantage in competitive climates yet hinder learning, full engagement and well-being,” Pope wrote.
Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school.
Their study found that too much homework is associated with:
* Greater stress: 56 percent of the students considered homework a primary source of stress, according to the survey data. Forty-three percent viewed tests as a primary stressor, while 33 percent put the pressure to get good grades in that category. Less than 1 percent of the students said homework was not a stressor.
* Reductions in health: In their open-ended answers, many students said their homework load led to sleep deprivation and other health problems. The researchers asked students whether they experienced health issues such as headaches, exhaustion, sleep deprivation, weight loss and stomach problems.
* Less time for friends, family and extracurricular pursuits: Both the survey data and student responses indicate that spending too much time on homework meant that students were “not meeting their developmental needs or cultivating other critical life skills,” according to the researchers. Students were more likely to drop activities, not see friends or family, and not pursue hobbies they enjoy.
A balancing act
The results offer empirical evidence that many students struggle to find balance between homework, extracurricular activities and social time, the researchers said. Many students felt forced or obligated to choose homework over developing other talents or skills.
Also, there was no relationship between the time spent on homework and how much the student enjoyed it. The research quoted students as saying they often do homework they see as “pointless” or “mindless” in order to keep their grades up.
“This kind of busy work, by its very nature, discourages learning and instead promotes doing homework simply to get points,” Pope said.
She said the research calls into question the value of assigning large amounts of homework in high-performing schools. Homework should not be simply assigned as a routine practice, she said.
“Rather, any homework assigned should have a purpose and benefit, and it should be designed to cultivate learning and development,” wrote Pope.
High-performing paradox
In places where students attend high-performing schools, too much homework can reduce their time to foster skills in the area of personal responsibility, the researchers concluded. “Young people are spending more time alone,” they wrote, “which means less time for family and fewer opportunities to engage in their communities.”
Student perspectives
The researchers say that while their open-ended or “self-reporting” methodology to gauge student concerns about homework may have limitations – some might regard it as an opportunity for “typical adolescent complaining” – it was important to learn firsthand what the students believe.
The paper was co-authored by Mollie Galloway from Lewis and Clark College and Jerusha Conner from Villanova University.
Media Contacts
Denise Pope, Stanford Graduate School of Education: (650) 725-7412, [email protected] Clifton B. Parker, Stanford News Service: (650) 725-0224, [email protected]
- Second Opinion
- Research & Innovation
- Patients & Families
- Health Professionals
- Recently Visited
- Segunda opinión
- Refer a patient
- MyChart Login
Healthier, Happy Lives Blog
Sort articles by..., sort by category.
- Celebrating Volunteers
- Community Outreach
- Construction Updates
- Family-Centered Care
- Healthy Eating
- Heart Center
- Interesting Things
- Mental Health
- Patient Stories
- Research and Innovation
- Safety Tips
- Sustainability
- World-Class Care
About Our Blog
- Back-to-School
- Pediatric Technology
Latest Posts
- Menstruation, Birth Control, Mental Health Top Team USA Female Athletes’ Research Agenda
- Two Sisters Return to the Bay Area to Work Together in the Johnson Center for Pregnancy and Newborn Services
- Heart-Lung Transplant Patient Going Strong, Reaching Dreams at 16-Year Mark
- Stanford Children’s Care Teams Invited to 49ers Training Camp as a Token of Gratitude
- Fortune Smiles on Couple Trying to Build a Family

Health Hazards of Homework
March 18, 2014 | Julie Greicius Pediatrics .

A new study by the Stanford Graduate School of Education and colleagues found that students in high-performing schools who did excessive hours of homework “experienced greater behavioral engagement in school but also more academic stress, physical health problems, and lack of balance in their lives.”
Those health problems ranged from stress, headaches, exhaustion, sleep deprivation, weight loss and stomach problems, to psycho-social effects like dropping activities, not seeing friends or family, and not pursuing hobbies they enjoy.
In the Stanford Report story about the research, Denise Pope , a senior lecturer at the Stanford Graduate School of Education and a co-author of the study published in the Journal of Experimental Education , says, “Our findings on the effects of homework challenge the traditional assumption that homework is inherently good.”
The study was based on survey data from a sample of 4,317 students from 10 high-performing high schools in California communities in which median household income exceeded $90,000. Of the students surveyed, homework volume averaged about 3.1 hours each night.
“It is time to re-evaluate how the school environment is preparing our high school student for today’s workplace,” says Neville Golden, MD , chief of adolescent medicine at Stanford Medicine Children’s Health and a professor at the School of Medicine. “This landmark study shows that excessive homework is counterproductive, leading to sleep deprivation, school stress and other health problems. Parents can best support their children in these demanding academic environments by advocating for them through direct communication with teachers and school administrators about homework load.”
Related Posts

Top-ranked group group in Los Gatos, Calif., is now a part of one of the…

The Stanford Medicine Children’s Health network continues to grow with our newest addition, Town and…
- Julie Greicius
- more by this author...
Connect with us:
Download our App:
ABOUT STANFORD MEDICINE CHILDREN'S HEALTH
- Leadership Team
- Vision, Mission & Values
- The Stanford Advantage
- Government and Community Relations
LUCILE PACKARD FOUNDATION FOR CHILDREN'S HEALTH
- Get Involved
- Volunteering Services
- Auxiliaries & Affiliates
- Our Hospital
- Send a Greeting Card
- New Hospital
- Refer a Patient
- Pay Your Bill
Also Find Us on:
- Notice of Nondiscrimination
- Terms of Use
- Privacy Policy
- Code of Conduct
- Price Transparency
- Stanford School of Medicine
- Stanford Health Care
- Stanford University
Is homework a necessary evil?
After decades of debate, researchers are still sorting out the truth about homework’s pros and cons. One point they can agree on: Quality assignments matter.
By Kirsten Weir
March 2016, Vol 47, No. 3
Print version: page 36

- Schools and Classrooms
Homework battles have raged for decades. For as long as kids have been whining about doing their homework, parents and education reformers have complained that homework's benefits are dubious. Meanwhile many teachers argue that take-home lessons are key to helping students learn. Now, as schools are shifting to the new (and hotly debated) Common Core curriculum standards, educators, administrators and researchers are turning a fresh eye toward the question of homework's value.
But when it comes to deciphering the research literature on the subject, homework is anything but an open book.
The 10-minute rule
In many ways, homework seems like common sense. Spend more time practicing multiplication or studying Spanish vocabulary and you should get better at math or Spanish. But it may not be that simple.
Homework can indeed produce academic benefits, such as increased understanding and retention of the material, says Duke University social psychologist Harris Cooper, PhD, one of the nation's leading homework researchers. But not all students benefit. In a review of studies published from 1987 to 2003, Cooper and his colleagues found that homework was linked to better test scores in high school and, to a lesser degree, in middle school. Yet they found only faint evidence that homework provided academic benefit in elementary school ( Review of Educational Research , 2006).
Then again, test scores aren't everything. Homework proponents also cite the nonacademic advantages it might confer, such as the development of personal responsibility, good study habits and time-management skills. But as to hard evidence of those benefits, "the jury is still out," says Mollie Galloway, PhD, associate professor of educational leadership at Lewis & Clark College in Portland, Oregon. "I think there's a focus on assigning homework because [teachers] think it has these positive outcomes for study skills and habits. But we don't know for sure that's the case."
Even when homework is helpful, there can be too much of a good thing. "There is a limit to how much kids can benefit from home study," Cooper says. He agrees with an oft-cited rule of thumb that students should do no more than 10 minutes a night per grade level — from about 10 minutes in first grade up to a maximum of about two hours in high school. Both the National Education Association and National Parent Teacher Association support that limit.
Beyond that point, kids don't absorb much useful information, Cooper says. In fact, too much homework can do more harm than good. Researchers have cited drawbacks, including boredom and burnout toward academic material, less time for family and extracurricular activities, lack of sleep and increased stress.
In a recent study of Spanish students, Rubén Fernández-Alonso, PhD, and colleagues found that students who were regularly assigned math and science homework scored higher on standardized tests. But when kids reported having more than 90 to 100 minutes of homework per day, scores declined ( Journal of Educational Psychology , 2015).
"At all grade levels, doing other things after school can have positive effects," Cooper says. "To the extent that homework denies access to other leisure and community activities, it's not serving the child's best interest."
Children of all ages need down time in order to thrive, says Denise Pope, PhD, a professor of education at Stanford University and a co-founder of Challenge Success, a program that partners with secondary schools to implement policies that improve students' academic engagement and well-being.
"Little kids and big kids need unstructured time for play each day," she says. Certainly, time for physical activity is important for kids' health and well-being. But even time spent on social media can help give busy kids' brains a break, she says.
All over the map
But are teachers sticking to the 10-minute rule? Studies attempting to quantify time spent on homework are all over the map, in part because of wide variations in methodology, Pope says.
A 2014 report by the Brookings Institution examined the question of homework, comparing data from a variety of sources. That report cited findings from a 2012 survey of first-year college students in which 38.4 percent reported spending six hours or more per week on homework during their last year of high school. That was down from 49.5 percent in 1986 ( The Brown Center Report on American Education , 2014).
The Brookings report also explored survey data from the National Assessment of Educational Progress, which asked 9-, 13- and 17-year-old students how much homework they'd done the previous night. They found that between 1984 and 2012, there was a slight increase in homework for 9-year-olds, but homework amounts for 13- and 17-year-olds stayed roughly the same, or even decreased slightly.
Yet other evidence suggests that some kids might be taking home much more work than they can handle. Robert Pressman, PhD, and colleagues recently investigated the 10-minute rule among more than 1,100 students, and found that elementary-school kids were receiving up to three times as much homework as recommended. As homework load increased, so did family stress, the researchers found ( American Journal of Family Therapy , 2015).
Many high school students also seem to be exceeding the recommended amounts of homework. Pope and Galloway recently surveyed more than 4,300 students from 10 high-achieving high schools. Students reported bringing home an average of just over three hours of homework nightly ( Journal of Experiential Education , 2013).
On the positive side, students who spent more time on homework in that study did report being more behaviorally engaged in school — for instance, giving more effort and paying more attention in class, Galloway says. But they were not more invested in the homework itself. They also reported greater academic stress and less time to balance family, friends and extracurricular activities. They experienced more physical health problems as well, such as headaches, stomach troubles and sleep deprivation. "Three hours per night is too much," Galloway says.
In the high-achieving schools Pope and Galloway studied, more than 90 percent of the students go on to college. There's often intense pressure to succeed academically, from both parents and peers. On top of that, kids in these communities are often overloaded with extracurricular activities, including sports and clubs. "They're very busy," Pope says. "Some kids have up to 40 hours a week — a full-time job's worth — of extracurricular activities." And homework is yet one more commitment on top of all the others.
"Homework has perennially acted as a source of stress for students, so that piece of it is not new," Galloway says. "But especially in upper-middle-class communities, where the focus is on getting ahead, I think the pressure on students has been ratcheted up."
Yet homework can be a problem at the other end of the socioeconomic spectrum as well. Kids from wealthier homes are more likely to have resources such as computers, Internet connections, dedicated areas to do schoolwork and parents who tend to be more educated and more available to help them with tricky assignments. Kids from disadvantaged homes are more likely to work at afterschool jobs, or to be home without supervision in the evenings while their parents work multiple jobs, says Lea Theodore, PhD, a professor of school psychology at the College of William and Mary in Williamsburg, Virginia. They are less likely to have computers or a quiet place to do homework in peace.
"Homework can highlight those inequities," she says.
Quantity vs. quality
One point researchers agree on is that for all students, homework quality matters. But too many kids are feeling a lack of engagement with their take-home assignments, many experts say. In Pope and Galloway's research, only 20 percent to 30 percent of students said they felt their homework was useful or meaningful.
"Students are assigned a lot of busywork. They're naming it as a primary stressor, but they don't feel it's supporting their learning," Galloway says.
"Homework that's busywork is not good for anyone," Cooper agrees. Still, he says, different subjects call for different kinds of assignments. "Things like vocabulary and spelling are learned through practice. Other kinds of courses require more integration of material and drawing on different skills."
But critics say those skills can be developed with many fewer hours of homework each week. Why assign 50 math problems, Pope asks, when 10 would be just as constructive? One Advanced Placement biology teacher she worked with through Challenge Success experimented with cutting his homework assignments by a third, and then by half. "Test scores didn't go down," she says. "You can have a rigorous course and not have a crazy homework load."
Still, changing the culture of homework won't be easy. Teachers-to-be get little instruction in homework during their training, Pope says. And despite some vocal parents arguing that kids bring home too much homework, many others get nervous if they think their child doesn't have enough. "Teachers feel pressured to give homework because parents expect it to come home," says Galloway. "When it doesn't, there's this idea that the school might not be doing its job."
Galloway argues teachers and school administrators need to set clear goals when it comes to homework — and parents and students should be in on the discussion, too. "It should be a broader conversation within the community, asking what's the purpose of homework? Why are we giving it? Who is it serving? Who is it not serving?"
Until schools and communities agree to take a hard look at those questions, those backpacks full of take-home assignments will probably keep stirring up more feelings than facts.
Further reading
- Cooper, H., Robinson, J. C., & Patall, E. A. (2006). Does homework improve academic achievement? A synthesis of research, 1987-2003. Review of Educational Research, 76 (1), 1–62. doi: 10.3102/00346543076001001
- Galloway, M., Connor, J., & Pope, D. (2013). Nonacademic effects of homework in privileged, high-performing high schools. The Journal of Experimental Education, 81 (4), 490–510. doi: 10.1080/00220973.2012.745469
- Pope, D., Brown, M., & Miles, S. (2015). Overloaded and underprepared: Strategies for stronger schools and healthy, successful kids . San Francisco, CA: Jossey-Bass.
Letters to the Editor
- Send us a letter
When Is Homework Stressful? Its Effects on Students’ Mental Health

Are you wondering when is homework stressful? Well, homework is a vital constituent in keeping students attentive to the course covered in a class. By applying the lessons, students learned in class, they can gain a mastery of the material by reflecting on it in greater detail and applying what they learned through homework.
However, students get advantages from homework, as it improves soft skills like organisation and time management which are important after high school. However, the additional work usually causes anxiety for both the parents and the child. As their load of homework accumulates, some students may find themselves growing more and more bored.
Students may take assistance online and ask someone to do my online homework . As there are many platforms available for the students such as Chegg, Scholarly Help, and Quizlet offering academic services that can assist students in completing their homework on time.
Negative impact of homework
There are the following reasons why is homework stressful and leads to depression for students and affect their mental health. As they work hard on their assignments for alarmingly long periods, students’ mental health is repeatedly put at risk. Here are some serious arguments against too much homework.
No uniqueness
Homework should be intended to encourage children to express themselves more creatively. Teachers must assign kids intriguing assignments that highlight their uniqueness. similar to writing an essay on a topic they enjoy.
Moreover, the key is encouraging the child instead of criticizing him for writing a poor essay so that he can express himself more creatively.
Lack of sleep
One of the most prevalent adverse effects of schoolwork is lack of sleep. The average student only gets about 5 hours of sleep per night since they stay up late to complete their homework, even though the body needs at least 7 hours of sleep every day. Lack of sleep has an impact on both mental and physical health.
No pleasure
Students learn more effectively while they are having fun. They typically learn things more quickly when their minds are not clouded by fear. However, the fear factor that most teachers introduce into homework causes kids to turn to unethical means of completing their assignments.
Excessive homework
The lack of coordination between teachers in the existing educational system is a concern. As a result, teachers frequently end up assigning children far more work than they can handle. In such circumstances, children turn to cheat on their schoolwork by either copying their friends’ work or using online resources that assist with homework.
Anxiety level
Homework stress can increase anxiety levels and that could hurt the blood pressure norms in young people . Do you know? Around 3.5% of young people in the USA have high blood pressure. So why is homework stressful for children when homework is meant to be enjoyable and something they look forward to doing? It is simple to reject this claim by asserting that schoolwork is never enjoyable, yet with some careful consideration and preparation, homework may become pleasurable.
No time for personal matters
Students that have an excessive amount of homework miss out on personal time. They can’t get enough enjoyment. There is little time left over for hobbies, interpersonal interaction with colleagues, and other activities.
However, many students dislike doing their assignments since they don’t have enough time. As they grow to detest it, they can stop learning. In any case, it has a significant negative impact on their mental health.
Children are no different than everyone else in need of a break. Weekends with no homework should be considered by schools so that kids have time to unwind and prepare for the coming week. Without a break, doing homework all week long might be stressful.
How do parents help kids with homework?
Encouraging children’s well-being and health begins with parents being involved in their children’s lives. By taking part in their homework routine, you can see any issues your child may be having and offer them the necessary support.
Set up a routine
Your student will develop and maintain good study habits if you have a clear and organized homework regimen. If there is still a lot of schoolwork to finish, try putting a time limit. Students must obtain regular, good sleep every single night.
Observe carefully
The student is ultimately responsible for their homework. Because of this, parents should only focus on ensuring that their children are on track with their assignments and leave it to the teacher to determine what skills the students have and have not learned in class.
Listen to your child
One of the nicest things a parent can do for their kids is to ask open-ended questions and listen to their responses. Many kids are reluctant to acknowledge they are struggling with their homework because they fear being labelled as failures or lazy if they do.
However, every parent wants their child to succeed to the best of their ability, but it’s crucial to be prepared to ease the pressure if your child starts to show signs of being overburdened with homework.
Talk to your teachers
Also, make sure to contact the teacher with any problems regarding your homework by phone or email. Additionally, it demonstrates to your student that you and their teacher are working together to further their education.
Homework with friends
If you are still thinking is homework stressful then It’s better to do homework with buddies because it gives them these advantages. Their stress is reduced by collaborating, interacting, and sharing with peers.
Additionally, students are more relaxed when they work on homework with pals. It makes even having too much homework manageable by ensuring they receive the support they require when working on the assignment. Additionally, it improves their communication abilities.
However, doing homework with friends guarantees that one learns how to communicate well and express themselves.
Review homework plan
Create a schedule for finishing schoolwork on time with your child. Every few weeks, review the strategy and make any necessary adjustments. Gratefully, more schools are making an effort to control the quantity of homework assigned to children to lessen the stress this produces.
Bottom line
Finally, be aware that homework-related stress is fairly prevalent and is likely to occasionally affect you or your student. Sometimes all you or your kid needs to calm down and get back on track is a brief moment of comfort. So if you are a student and wondering if is homework stressful then you must go through this blog.
While homework is a crucial component of a student’s education, when kids are overwhelmed by the amount of work they have to perform, the advantages of homework can be lost and grades can suffer. Finding a balance that ensures students understand the material covered in class without becoming overburdened is therefore essential.
Zuella Montemayor did her degree in psychology at the University of Toronto. She is interested in mental health, wellness, and lifestyle.
Psychreg is a digital media company and not a clinical company. Our content does not constitute a medical or psychological consultation. See a certified medical or mental health professional for diagnosis.
- Privacy Policy
© Copyright 2014–2034 Psychreg Ltd
- PSYCHREG JOURNAL
- MEET OUR WRITERS
- MEET THE TEAM

Does Homework Serve a Purpose?
Finding the right balance between schoolwork and home life..
Posted November 5, 2018 | Reviewed by Ekua Hagan
- What Is Stress?
- Take our Burnout Test
- Find a therapist to overcome stress

Homework — a dreaded word that means more work and less play. The mere thought of doing additional work after a seven-hour day (that begins extremely early) can be gruesome. Not to mention, many teens have other commitments after the school day ends.
According to the U.S. Census Bureau, nearly 57 percent of children between the ages of 6 and 17 years old participate in at least one after-school extracurricular activity. And that’s a good thing because youth extracurricular involvement comes with benefits such as boosting academic performance, reducing risky behaviors (i.e., drug use and drinking), promoting physical health, and providing a safe structured environment. However, tag these extracurricular activities onto the end of a school day and you’ll find that many teens don’t get home until it's dark outside.
What about the teen who works a 15- to 20-hour job on top of an extracurricular activity? The US Department of Labor reports that one in five high school students have a part-time job, and those jobs too can come with added benefits. Teens who work often learn the value of a hard-earned dollar. They learn how to manage their money, learn to problem solve, and most importantly, they learn how to work with people. Plus, a job in high school is a great way to add valuable experience to a resume.
With so many after school opportunities available for teens, it can be extremely difficult for them to balance homework with their other commitments. Oftentimes, active kids simply don’t have enough time in a day to get all that’s asked of them finished. When it comes homework, in all my years of working in the public school system, I have never seen a student jump for joy when homework was assigned. Of course, there are some who were anxious to complete the assignment, but that was more to get it off their busy plate. Which brings us to the essential question — does homework serve a purpose?
There are those who stand firm and back the claim that homework does serve a purpose . They often cite that homework helps prepare students for standardized tests, that it helps supplement and reinforce what’s being taught in class, and that it helps teach fundamental skills such as time management , organization, task completion, as well as responsibility (extracurricular activities and work experience can also teach those fundamental skills).
Another argument for homework is that having students complete work independently shows that they can demonstrate mastery of the material without the assistance of a teacher. Additionally, there have been numerous studies supporting homework, like a recent study that shows using online systems to assign math homework has been linked to a statistically significant boost in test scores. So, there you have it: Homework has a lot of perks and one of those involves higher test scores, particularly in math. But don’t form your opinion just yet.
Although many people rally for and support homework, there is another school of thought that homework should be decreased, or better yet, abolished. Those who join this group often cite studies linking academic stress to health risks. For example, one study in the Journal of Educational Psychology showed that when middle school students were assigned more than 90 to 100 minutes of daily homework, their math and science test scores began to decline.

The Journal of Experimental Education published research indicating that when high school students were assigned too much homework, they were more susceptible to serious mental and physical health problems, high-stress levels, and sleep deprivation. Stanford University also did a study that showed more than a couple of hours of homework a night was counterproductive. Think about it — teens spend an entire day at school, followed by extracurricular activities and possibly work, and then they get to end their day with two to three hours of homework. Now that’s a long day! No wonder so many of our teens are sleep-deprived and addicted to caffeine? On average most teens only get about 7.4 hours of sleep per night but according to the American Academy of Pediatrics , they need 8 to 10 hours.
Regardless of where you stand on the homework debate, a few things are certain: If homework is given, it should be a tool that’s used to enhance learning. Also, teachers should take into account the financial requirements of assignments, electronic accessibility, and they should be familiar with student needs as well as their other commitments. For example, not all students have equal opportunities to finish their homework, so incomplete work may not be a true reflection of their ability—it may be the result of other issues they face outside of school.
Many of today's teens are taking college-level courses as early as the ninth and tenth grades. With the push of programs such as Advanced Placement, International Baccalaureate, Early College Programs, and Dual Enrollment, today’s teens are carrying academic loads that surpass past generations. The result of this push for rigor can lead to high levels of stress, exhaustion, sleep deprivation, depression , anxiety , and early burnout . Too many teens are already running on empty. With more than half of teens reporting school and homework as a primary source of their stress, it’s evident that academic pressure is becoming a burden.

On the flip side, not all students spend a lot of time doing homework. What takes one student an hour to complete may take another three hours. Too often educators don’t take this into account when assigning homework. According to the University of Phoenix College of Education teacher survey, high school students can get assigned up to 17.5 hours of homework each week. To top it off, a Today article reported that teachers often underestimate the amount of homework they assign by as much as 50%. Now that’s a huge miscalculation, and our nation's youth have to suffer the consequences of those errors.

There are definitely pros and cons to doing homework. I think the bigger question that educators need to address is, “what’s the purpose of the assignment?” Is it merely a way to show parents and administration what's going on in the class? Is it a means to help keep students' grades afloat by giving a grade for completion or is the assignment being graded for accuracy? Does the assignment enhance and supplement the learning experience? Furthermore, is it meaningful or busywork?
The homework debate will likely continue until we take a good, hard look at our current policies and practices. What side of the line do you stand on when it comes to homework? Perhaps you’re somewhere in the middle?
Please weigh in with your thoughts. I am always eager to hear students’ voices in this discussion. If you are a student, please share what’s on your plate and how much time you spend doing homework each night.
Challenge Success White Paper: http://www.challengesuccess.org/wp-content/uploads/2015/07/ChallengeSuc…
Cooper, H., et al. (meta analysis): https://www.jstor.org/stable/3700582?seq=1#page_scan_tab_contents
Marzano, R., et al.: http://www.marzanocenter.com/2013/01/17/have-you-done-your-homework-on-…
NEA (National Education Association): http://www.nea.org/tools/16938.htm
Pope, Brown, and Miles (2015), Overloaded and Underprepared. (Brief synopsis here: https://www.learningandthebrain.com/blog/overloaded-and-underprepared-s… )

Raychelle Cassada Lohman n , M.S., LPC, is the author of The Anger Workbook for Teens .
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Online Therapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Self Tests NEW
- Therapy Center
- Diagnosis Dictionary
- Types of Therapy

Sticking up for yourself is no easy task. But there are concrete skills you can use to hone your assertiveness and advocate for yourself.
- Emotional Intelligence
- Gaslighting
- Affective Forecasting
- Neuroscience
You are using an outdated browser. Please upgrade your browser to improve your experience.
Suggested Results
- EdCommunities
- NEA Foundation
Study: Too Many Enrichment Activities Harm Mental Health
By: Tim Walker , Senior Writer Published: March 31, 2024
Even before the pandemic, U.S. students were struggling with mental health. But the statistics have since become even more alarming. According to a new federal of teen health , about 1 in 5 adolescents report symptoms of anxiety or depression.
The impact of social media and bullying have, for good reason, dominated much of the discussion around this growing crisis. But there are other factors that increase student stress and anxiety that are not as widely reported, including not getting enough downtime.
Homework is at least partly to blame. Despite being under increased scrutiny over the past decade or so, homework is still a pillar of many U.S. classrooms. While educators and other experts have questioned its value, especially in the lower grades, others believe that homework can enhance instruction and keep students engaged if assigned in moderation. Too much homework, on the other hand, is something else entirely. The academic benefits can be marginal and too many assignments are a source of stress.
But what about other enrichment activities and extra-curriculars that are designed to bolster a child’s education (and, for high school students, college applications), such as sports, tutoring, clubs, before- and after-school programs. Is there such a thing as too much?
Yes, according to a new study by researchers at the University of Georgia. Too many enrichment activities can result in an “overscheduled” student, and that can have adverse effects—namely heightened stress and anxiety— particularly at the high school level.
There are only so many hours in a day. If they are consumed by extra assignments and activities, the student has less time to spend on developing non-cognitive or "soft" skills—skills that can be aided by relaxing, socializing and—yes, even sleeping.
Furthermore, the academic outcomes that homework and other enrichment activities are designed to bolster are overhyped. Beyond a certain point, the effect is “basically zero,” says Carolina Caetano, one of the study’s authors and an assistant professor of economics at the University of Georgia. Caetano and her colleagues found that students are assigned so much homework and signed up for so many extracurricular activities that the “last hour” was no longer helping to build their academic skills.
So the cognitive benefits flatline while student mental health is being jeopardized.
“It’s not that these assignments and activities have no value,” says Caetano. “But a threshold can be reached in which the effects turn negative. There's quite a lot of pressure on these kids from all corners. They’re undertaking much more than they really should when they probably should, at this point, just be spending more time with friends and just being free.”
Declining Academic Benefits, More Stress
For the study, the researchers analyzed the time diaries from 4,300 K-12 students, collected as part of the Child Development Supplement of the Panel Study of Income Dynamics . With this data, they could see how much time was spent per week on certain activities.
The researchers then compared time spent on these activities with academic achievement. They also held them up against psychological measures, such as being withdrawn, anxious or angry. This data was taken from parent surveys about their children’s behavior.
On average, children in the sample spent about forty-five minutes per day on enrichment activities, but that adds up over a typical week. At first, there is a clear connection between enrichment activities, academic achievement, and positive behaviors. But sure enough, at a certain point, the academic benefits decline while the problems in well-being begin to ratchet up.
These negative effects were visible and significant across all grade levels but were more prevalent in high schoolers—likely due to their heavier homework load and the added pressure of college admissions.
“The older kids do substantially more homework and substantially more of the academic type of activity,” Caetano explains. “The younger kids do a lot more of the sports and arts classes.”
Still, many elementary students are over-scheduled. If there was less on their plate, they may be allowed to enjoy more free time and become more adept at developing softer skills by the time they reach high school.
So what is the solution? That is tricky because over-scheduling students is a societal problem. “Homework is not assigned by parents. There are activities colleges demand in their candidates. It's not all a private decision made by the family.”
At the same time, even as educators point out the role homework plays in stress, not to mention the questionable academic value, many parents may still be hesitant to see it fall be the wayside or be dramatically scaled back. Homework can allow parents to understand what their students are learning and provides an opportunity to be more engaged in that work.
“Teachers should engage parents on this issue, educate them on the research that demonstrates that a lot of homework is not useful or healthy,” Caetano says. “And everyone—colleges, schools and parents—needs to understand the value of non-cognitive skills and how emotional well-being affects future success and happiness.”
Related Content
Stigma buster: schools look at mental health days for students, will the pandemic change homework forever, are schools ready to tackle the mental health crisis, reference s.
- 1 Election 2024: Education on the Ballot
- 2 Education Support Professionals Often First to See Student Mental Health Struggles
- 3 Recess During the Pandemic: More Important Than Ever
- 1 Resolution Ensuring Safe and Just Schools for All Students
- 2 NEA’s School Crisis Guide
- 3 ESP Webinar: Wellness Skills for Self-care and Health for Educational Support Professionals
Resources to Support Student & Educator Mental Health
Get more from, great public schools for every student.
This site uses various technologies, as described in our Privacy Policy, for personalization, measuring website use/performance, and targeted advertising, which may include storing and sharing information about your site visit with third parties. By continuing to use this website you consent to our Privacy Policy and Terms of Use .
We are experiencing sporadically slow performance in our online tools, which you may notice when working in your dashboard. Our team is fully engaged and actively working to improve your online experience. If you are experiencing a connectivity issue, we recommend you try again in 10-15 minutes. We will update this space when the issue is resolved.
Enter your email to unlock an extra $25 off an SAT or ACT program!
By submitting my email address. i certify that i am 13 years of age or older, agree to recieve marketing email messages from the princeton review, and agree to terms of use., homework wars: high school workloads, student stress, and how parents can help.

Studies of typical homework loads vary : In one, a Stanford researcher found that more than two hours of homework a night may be counterproductive. The research , conducted among students from 10 high-performing high schools in upper-middle-class California communities, found that too much homework resulted in stress, physical health problems and a general lack of balance.
Additionally, the 2014 Brown Center Report on American Education , found that with the exception of nine-year-olds, the amount of homework schools assign has remained relatively unchanged since 1984, meaning even those in charge of the curricula don't see a need for adding more to that workload.
But student experiences don’t always match these results. On our own Student Life in America survey, over 50% of students reported feeling stressed, 25% reported that homework was their biggest source of stress, and on average teens are spending one-third of their study time feeling stressed, anxious, or stuck.
The disparity can be explained in one of the conclusions regarding the Brown Report:
Of the three age groups, 17-year-olds have the most bifurcated distribution of the homework burden. They have the largest percentage of kids with no homework (especially when the homework shirkers are added in) and the largest percentage with more than two hours.
So what does that mean for parents who still endure the homework wars at home?
Read More: Teaching Your Kids How To Deal with School Stress
It means that sometimes kids who are on a rigorous college-prep track, probably are receiving more homework, but the statistics are melding it with the kids who are receiving no homework. And on our survey, 64% of students reported that their parents couldn’t help them with their work. This is where the real homework wars lie—not just the amount, but the ability to successfully complete assignments and feel success.
Parents want to figure out how to help their children manage their homework stress and learn the material.
Our Top 4 Tips for Ending Homework Wars
1. have a routine..
Every parenting advice article you will ever read emphasizes the importance of a routine. There’s a reason for that: it works. A routine helps put order into an often disorderly world. It removes the thinking and arguing and “when should I start?” because that decision has already been made. While routines must be flexible to accommodate soccer practice on Tuesday and volunteer work on Thursday, knowing in general when and where you, or your child, will do homework literally removes half the battle.
2. Have a battle plan.
Overwhelmed students look at a mountain of homework and think “insurmountable.” But parents can look at it with an outsider’s perspective and help them plan. Put in an extra hour Monday when you don’t have soccer. Prepare for the AP Chem test on Friday a little at a time each evening so Thursday doesn’t loom as a scary study night (consistency and repetition will also help lock the information in your brain). Start reading the book for your English report so that it’s underway. Go ahead and write a few sentences, so you don’t have a blank page staring at you. Knowing what the week will look like helps you keep calm and carry on.
3. Don’t be afraid to call in reserves.
You can’t outsource the “battle” but you can outsource the help ! We find that kids just do better having someone other than their parents help them —and sometimes even parents with the best of intentions aren’t equipped to wrestle with complicated physics problem. At The Princeton Review, we specialize in making homework time less stressful. Our tutors are available 24/7 to work one-to-one in an online classroom with a chat feature, interactive whiteboard, and the file sharing tool, where students can share their most challenging assignments.
4. Celebrate victories—and know when to surrender.
Students and parents can review completed assignments together at the end of the night -- acknowledging even small wins helps build a sense of accomplishment. If you’ve been through a particularly tough battle, you’ll also want to reach reach a cease-fire before hitting your bunk. A war ends when one person disengages. At some point, after parents have provided a listening ear, planning, and support, they have to let natural consequences take their course. And taking a step back--and removing any pressure a parent may be inadvertently creating--can be just what’s needed.
Stuck on homework?
Try an online tutoring session with one of our experts, and get homework help in 40+ subjects.
Try a Free Session

Explore Colleges For You
Connect with our featured colleges to find schools that both match your interests and are looking for students like you.

Career Quiz
Take our short quiz to learn which is the right career for you.

Get Started on Athletic Scholarships & Recruiting!
Join athletes who were discovered, recruited & often received scholarships after connecting with NCSA's 42,000 strong network of coaches.

Best 389 Colleges
165,000 students rate everything from their professors to their campus social scene.
SAT Prep Courses
1400+ course, act prep courses, free sat practice test & events, 1-800-2review, free digital sat prep try our self-paced plus program - for free, get a 14 day trial.

Free MCAT Practice Test
I already know my score.

MCAT Self-Paced 14-Day Free Trial

Enrollment Advisor
1-800-2REVIEW (800-273-8439) ext. 1
1-877-LEARN-30
Mon-Fri 9AM-10PM ET
Sat-Sun 9AM-8PM ET
Student Support
1-800-2REVIEW (800-273-8439) ext. 2
Mon-Fri 9AM-9PM ET
Sat-Sun 8:30AM-5PM ET
Partnerships
- Teach or Tutor for Us
College Readiness
International
Advertising
Affiliate/Other
- Enrollment Terms & Conditions
- Accessibility
- Cigna Medical Transparency in Coverage
Register Book
Local Offices: Mon-Fri 9AM-6PM
- SAT Subject Tests
Academic Subjects
- Social Studies
Find the Right College
- College Rankings
- College Advice
- Applying to College
- Financial Aid
School & District Partnerships
- Professional Development
- Advice Articles
- Private Tutoring
- Mobile Apps
- International Offices
- Work for Us
- Affiliate Program
- Partner with Us
- Advertise with Us
- International Partnerships
- Our Guarantees
- Accessibility – Canada
Privacy Policy | CA Privacy Notice | Do Not Sell or Share My Personal Information | Your Opt-Out Rights | Terms of Use | Site Map
©2024 TPR Education IP Holdings, LLC. All Rights Reserved. The Princeton Review is not affiliated with Princeton University
TPR Education, LLC (doing business as “The Princeton Review”) is controlled by Primavera Holdings Limited, a firm owned by Chinese nationals with a principal place of business in Hong Kong, China.
share this!
August 16, 2021
Is it time to get rid of homework? Mental health experts weigh in
by Sara M Moniuszko
It's no secret that kids hate homework. And as students grapple with an ongoing pandemic that has had a wide-range of mental health impacts, is it time schools start listening to their pleas over workloads?
Some teachers are turning to social media to take a stand against homework .
Tiktok user @misguided.teacher says he doesn't assign it because the "whole premise of homework is flawed."
For starters, he says he can't grade work on "even playing fields" when students' home environments can be vastly different.
"Even students who go home to a peaceful house, do they really want to spend their time on busy work? Because typically that's what a lot of homework is, it's busy work," he says in the video that has garnered 1.6 million likes. "You only get one year to be 7, you only got one year to be 10, you only get one year to be 16, 18."
Mental health experts agree heavy work loads have the potential do more harm than good for students, especially when taking into account the impacts of the pandemic. But they also say the answer may not be to eliminate homework altogether.
Emmy Kang, mental health counselor at Humantold, says studies have shown heavy workloads can be "detrimental" for students and cause a "big impact on their mental, physical and emotional health."
"More than half of students say that homework is their primary source of stress, and we know what stress can do on our bodies," she says, adding that staying up late to finish assignments also leads to disrupted sleep and exhaustion.
Cynthia Catchings, a licensed clinical social worker and therapist at Talkspace, says heavy workloads can also cause serious mental health problems in the long run, like anxiety and depression.
And for all the distress homework causes, it's not as useful as many may think, says Dr. Nicholas Kardaras, a psychologist and CEO of Omega Recovery treatment center.
"The research shows that there's really limited benefit of homework for elementary age students, that really the school work should be contained in the classroom," he says.
For older students, Kang says homework benefits plateau at about two hours per night.
"Most students, especially at these high-achieving schools, they're doing a minimum of three hours, and it's taking away time from their friends from their families, their extracurricular activities. And these are all very important things for a person's mental and emotional health."
Catchings, who also taught third to 12th graders for 12 years, says she's seen the positive effects of a no homework policy while working with students abroad.
"Not having homework was something that I always admired from the French students (and) the French schools, because that was helping the students to really have the time off and really disconnect from school ," she says.
The answer may not be to eliminate homework completely, but to be more mindful of the type of work students go home with, suggests Kang, who was a high-school teacher for 10 years.
"I don't think (we) should scrap homework, I think we should scrap meaningless, purposeless busy work-type homework. That's something that needs to be scrapped entirely," she says, encouraging teachers to be thoughtful and consider the amount of time it would take for students to complete assignments.
The pandemic made the conversation around homework more crucial
Mindfulness surrounding homework is especially important in the context of the last two years. Many students will be struggling with mental health issues that were brought on or worsened by the pandemic, making heavy workloads even harder to balance.
"COVID was just a disaster in terms of the lack of structure. Everything just deteriorated," Kardaras says, pointing to an increase in cognitive issues and decrease in attention spans among students. "School acts as an anchor for a lot of children, as a stabilizing force, and that disappeared."
But even if students transition back to the structure of in-person classes, Kardaras suspects students may still struggle after two school years of shifted schedules and disrupted sleeping habits.
"We've seen adults struggling to go back to in-person work environments from remote work environments. That effect is amplified with children because children have less resources to be able to cope with those transitions than adults do," he explains.
'Get organized' ahead of back-to-school
In order to make the transition back to in-person school easier, Kang encourages students to "get good sleep, exercise regularly (and) eat a healthy diet."
To help manage workloads, she suggests students "get organized."
"There's so much mental clutter up there when you're disorganized... sitting down and planning out their study schedules can really help manage their time," she says.
Breaking assignments up can also make things easier to tackle.
"I know that heavy workloads can be stressful, but if you sit down and you break down that studying into smaller chunks, they're much more manageable."
If workloads are still too much, Kang encourages students to advocate for themselves.
"They should tell their teachers when a homework assignment just took too much time or if it was too difficult for them to do on their own," she says. "It's good to speak up and ask those questions. Respectfully, of course, because these are your teachers. But still, I think sometimes teachers themselves need this feedback from their students."
©2021 USA Today Distributed by Tribune Content Agency, LLC.
Explore further
Feedback to editors

Scientists cook up a plan to save freshwater crocodiles from toxic cane toads
8 hours ago

Climate change raised the odds of unprecedented wildfires in 2023–24, say scientists
9 hours ago

Advanced microscopy method reveals hidden world of nanoscale optical metamaterials

New interpretation of runic inscription reveals pricing in Viking Age
10 hours ago

AI, computation, and the folds of life: Supercomputers help train a software tool for the protein modeling community

'Mirror' nuclei help connect nuclear theory and neutron stars

The atmosphere in the room can affect strategic decision-making, study finds

Coherence entropy unlocks new insights into light-field behavior
11 hours ago

Research team finds evidence of hydration on the asteroid Psyche

Scientists achieve more than 98% efficiency in removing nanoplastics from water
Relevant physicsforums posts, free abstract algebra curriculum in urdu and hindi.
2 hours ago
Incandescent bulbs in teaching
Aug 12, 2024
Sources to study basic logic for precocious 10-year old?
Jul 21, 2024
Kumon Math and Similar Programs
Jul 19, 2024
AAPT 2024 Summer Meeting Boston, MA (July 2024) - are you going?
Jul 4, 2024
How is Physics taught without Calculus?
Jun 25, 2024
More from STEM Educators and Teaching
Related Stories

Smartphones are lowering student's grades, study finds
Aug 18, 2020

Doing homework is associated with change in students' personality
Oct 6, 2017

Scholar suggests ways to craft more effective homework assignments
Oct 1, 2015

Should parents help their kids with homework?
Aug 29, 2019

How much math, science homework is too much?
Mar 23, 2015

Anxiety, depression, burnout rising as college students prepare to return to campus
Jul 26, 2021
Recommended for you

The 'knowledge curse': More isn't necessarily better
Aug 7, 2024

Visiting an art exhibition can make you think more socially and openly—but for how long?
Aug 6, 2024

Autonomy boosts college student attendance and performance
Jul 31, 2024

Study reveals young scientists face career hurdles in interdisciplinary research
Jul 29, 2024

Transforming higher education for minority students: Minor adjustments, major impacts

Communicating numbers boosts trust in climate change science, research suggests
Jul 26, 2024
Let us know if there is a problem with our content
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Phys.org in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
- Close Menu Search
- Recommend a Story

The Lion's Roar
May 24 Party Like It’s 1989: Lions Capture the 2024 Diamond Classic
May 24 Why Does the Early 20th Century Tend to Spark Nostalgia?
May 24 O.J Simpson Dead at 76: Football Star Turned Murderer
May 24 NAIA Bans Transgender Women From Women’s Sports
May 24 From Papyrus to Ashes: The Story of the Great Library of Alexandria
How Homework Is Destroying Teens’ Health
Jessica Amabile '24 , Staff Writer March 25, 2022
“[Students] average about 3.1 hours of homework each night,” according to an article published by Stanford . Teens across the country come home from school, exhausted from a long day, only to do more schoolwork. They sit at their computers, working on homework assignments for hours on end. To say the relentless amount of work they have to do is overwhelming would be an understatement. The sheer amount of homework given has many negative impacts on teenagers.
Students have had homework for decades, but in more recent years it has become increasingly more demanding. Multiple studies have shown that students average about three hours of homework per night. The Atlantic mentioned that students now have twice as much homework as students did in the 1990s. This is extremely detrimental to teens’ mental health and levels of stress. Students have a lot to do after school, such as spending time with family, extracurricular activities, taking care of siblings or other family members, hanging out with friends, or all of the above. Having to juggle all of this as well as hours on end of homework is unreasonable because teenagers already have enough to think or worry about.
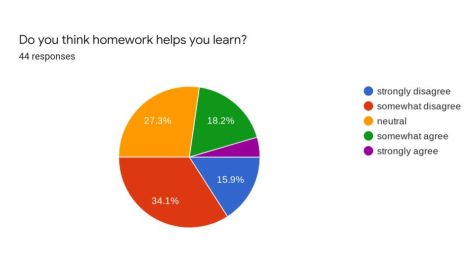
According to a student- run survey conducted in Cherry Hill West, students reported that they received the most homework in math, history, and language arts classes. They receive anywhere from 1 to 4 or more hours of homework every day, but only about 22.7% somewhat or strongly agree that it helps them learn. Of the students who participated, 63.6% think schools should continue to give out homework sometimes, while 27.3% said they should not give out homework at all. In an open-ended response section, students had a lot to say. One student wrote, “I think we should get homework to practice work if we are seen struggling, or didn’t finish work in class. But if we get homework, I think it just shows that the teacher needs more time to teach and instead of speeding up, gives us more work.” Another added, “Homework is important to learn the material. However, too much may lead to the student not learning that much, or it may become stressful to do homework everyday.” Others wrote, “The work I get in chemistry doesn’t help me learn at all if anything it confuses me more,” and “I think math is the only class I could use homework as that helps me learn while world language is supposed to help me learn but feels more like a time waste.” A student admitted, “I think homework is beneficial for students but the amount of homework teachers give us each day is very overwhelming and puts a lot of stress on kids. I always have my work done but all of the homework I have really changes my emotions and it effects me.” Another pointed out, “you are at school for most of your day waking up before the sun and still after all of that they send you home each day with work you need to do before the next day. Does that really make sense[?]”
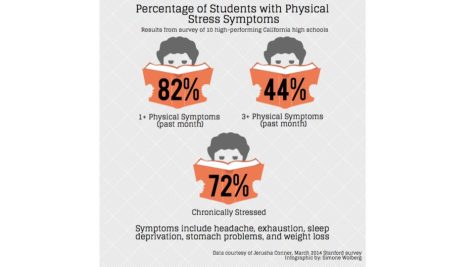
As an article from Healthline mentioned, “Researchers asked students whether they experienced physical symptoms of stress… More than 80 percent of students reported having at least one stress-related symptom in the past month, and 44 percent said they had experienced three or more symptoms.” If school is causing students physical symptoms of stress, it needs to re-evaluate whether or not homework is beneficial to students, especially teenagers. Students aren’t learning anything if they have hours of “busy work” every night, so much so that it gives them symptoms of stress, such as headaches, weight loss, sleep deprivation, and so on. The continuous hours of work are doing nothing but harming students mentally and physically.

The mental effects of homework can be harmful as well. Mental health issues are often ignored, even when schools can be the root of the problem. An article from USA Today contained a quote from a licensed therapist and social worker named Cynthia Catchings, which reads, “ heavy workloads can also cause serious mental health problems in the long run, like anxiety and depression.” Mental health problems are not beneficial in any way to education. In fact, it makes it more difficult for students to focus and learn.
Some studies have suggested that students should receive less homework. To an extent, homework can help students in certain areas, such as math. However, too much has detrimental impacts on their mental and physical health. Emmy Kang, a mental health counselor, has a suggestion. She mentioned, “I don’t think (we) should scrap homework; I think we should scrap meaningless, purposeless busy work-type homework. That’s something that needs to be scrapped entirely,” she says, encouraging teachers to be thoughtful and consider the amount of time it would take for students to complete assignments,” according to USA Today . Students don’t have much control over the homework they receive, but if enough people could explain to teachers the negative impacts it has on them, they might be convinced. Teachers need to realize that their students have other classes and other assignments to do. While this may not work for everything, it would at least be a start, which would be beneficial to students.
The sole purpose of schools is to educate children and young adults to help them later on in life. However, school curriculums have gone too far if hours of homework for each class are seen as necessary and beneficial to learning. Many studies have shown that homework has harmful effects on students, so how does it make sense to keep assigning it? At this rate, the amount of time spent on homework will increase in years to come, along with the effects of poor mental and physical health. Currently, students do an average of 3 hours of homework, according to the Washington Post, and the estimated amount of teenagers suffering from at least one mental illness is 1 in 5, as Polaris Teen Center stated. This is already bad enough–it’s worrisome to think it could get much worse. Homework is not more important than physical or mental health, by any standards.
What time should high school should start?
- 7:00 AM or earlier
- 7:30 AM (Current Start Time)
- After 9:00 AM
View Results
- Polls Archive
Comments (0)
Cancel reply
Your email address will not be published. Required fields are marked *

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Wiley Open Access Collection
Mental health effects of education
Fjolla kondirolli.
1 University of Sussex, Brighton UK
Naveen Sunder
2 Bentley University, Waltham Massachusetts, USA
Associated Data
World Health Survey data is available online at https://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/whs/about . Demographic and Health Surveys data is available online at https://dhsprogram.com/ . Zimbabwe census data is available online at https://www.zimstat.co.zw/ .
We analyze the role of education as a determinant of mental health. To do this, we leverage the age‐specific exposure to an educational reform as an instrument for years of education and find that the treated cohorts gained more education. This increase in education had an effect on mental health more than 2 decades later. An extra year of education led to a lower likelihood of reporting any symptoms related to depression (11.3%) and anxiety (9.8%). More educated people also suffered less severe symptoms – depression (6.1%) and anxiety (5.6%). These protective effects are higher among women and rural residents. The effects of education on mental well‐being that we document are potentially mediated through better physical health, improved health behavior and knowledge, and an increase in women's empowerment.
1. INTRODUCTION
Mental health accounts for around seven percent of the global disease burden and 19% of all disability years (James, 2018 ; Rehm & Shield, 2019 ). In addition to being a valuable end in itself, mental well‐being is critical because it is a key determinant of a number of socio‐economic outcomes such as premature mortality (Graham & Pinto, 2019 ) and lower life expectancy (Wahlbeck et al., 2011 ), and higher risk of other communicable and non‐communicable diseases (Hobkirk et al., 2015 ; Prince et al., 2007 ). In terms of economic outcomes, people with lower psychological well‐being have a higher likelihood of being unemployed (Frijters et al., 2014 ), earn lower wages (Graham et al., 2004 ), and are less productive (Oswald et al., 2015 ). This makes them vulnerable to economic shocks and more likely to live in poverty (Lund et al., 2011 ).
The negative effects of poor mental health are exacerbated in low‐ and middle‐income countries due to under‐treatment. Estimates suggest that under‐treatment is around 76–90% in low and middle‐income countries as opposed to 35–50% in developed countries (Patel et al., 2010 ). Mental health is stigmatized in low‐income countries – evidence from a variety of contexts including Ethiopia (Shibre et al., 2001 ), India (Koschorke et al., 2014 ), and Nigeria (Oshodi et al., 2014 ) demonstrates that individuals suffering from poor mental health fear being discriminated against and being ostracized by society, and consequently under‐report these issues and have a lower likelihood of seeking appropriate treatment. The under‐reporting of mental health issues, coupled with low investment in mental health infrastructure and diminished availability of human resources results in a higher treatment gap in these countries (Mascayano et al., 2015 ). The high prevalence and low rates of treatment of mental disorders in developing countries creates a large welfare loss ‐ Bloom et al. ( 2011 ) estimate that by the year 2030, mental disorders are expected to lead to a loss in economic output amounting to around 20% of the global GDP. This necessitates the need to study factors that can help improve mental health. We explore the role of one such factor – education.
In particular, we examine the effect of years of education on long‐run mental health of individuals. We do so in the context of Zimbabwe. Before 1980, the country was under British colonial rule, and there were several discriminatory policies that restricted educational attainment among Black Zimbabweans. For example, primary education (grades 1–7) was free and compulsory only for White students, while Black students had to pay fees and were not required to enroll. Black students also had to take a competitive exam (for a limited number of seats) to gain admission into secondary school, while their White counterparts received automatic progression. Post‐independence (in 1980) the new government focused their efforts on improving educational outcomes, and implemented three critical reforms ‐ (1) free and compulsory primary education for all, (2) automatic progression into secondary school, and (3) the relaxing of age restrictions related to entry into primary school. These reforms benefited Black children who were of primary school‐going age at the time. Since Zimbabwean kids started school when they turned six, those who were 13 years or younger in 1980 disproportionately benefited from these policies (treatment group). Since the reform also allowed for some over‐age students to enroll in school, some children who were 14 or 15 years of age in 1980 might have also experienced some educational gains (the partially treated group). However, older individuals (16 years or above at the time) were significantly less likely to experience any such benefits, 1 and thus form our control group.
We utilize this age‐specific exposure to an educational reform in Zimbabwe in the 1980s as an instrumental variable (IV) for years of education to estimate the causal effect of schooling on later life mental health. We use an age cutoff of 15 years to define reform exposure – those who were 15 years and below in 1980 form the treated group, while those 16 years and older are considered as untreated. Our identification strategy rests on the assumption that individuals on either side of the age cutoff were, on average, conditionally indistinguishable, except for their exposure to this education policy, which led to higher levels of education among the treated. Our results indicate that the treated group eventually gained about three years of education and were 39% points more likely to attend secondary school. Our IV results suggest that this enhanced education led to better mental health later in life. We find significant effects of education on both the likelihood of having any adverse mental health related symptoms, and the severity of these symptoms. An extra year of schooling reduced the probability of reporting any symptoms related to depression (11.3%) or anxiety (9.8%) in adult life, and it also led to a decline in the severity of symptoms of both depression (6.1%), and anxiety (5.6%). Our findings suggest that the effects are larger among women and rural residents. We find evidence that improved physical health, better health‐related behavior and an increase in female empowerment might be some of the mechanisms through which education might have shaped mental health in the Zimbabwean context. We conduct a number of sensitivity analyses to show that our results are robust to various modifications in the empirical strategy, including levels at which the standard errors are clustered, and choice of bandwidth.
This paper contributes to two separate strands of literature. First, it adds to the growing evidence on the link between education and mental health. 2 While some studies find a positive impact of education on mental well‐being (Chevalier & Feinstein, 2006 ; Courtin et al., 2019 ; Crespo et al., 2014 ; Dursun & Cesur, 2016 ; Jiang et al., 2020 ; Lager et al., 2017 ; Li & Sunder, 2022 ; Mazzonna, 2014 ; Wang, 2021 ), others document a negative effect (Avendano et al., 2020 ) or null effects (Begerow & Jürges, 2021 ; Böckerman et al., 2021 ). In addition to the mixed results of education on mental health, the bulk of this literature is based on developed countries, such as the UK, USA, Canada, Germany, and Sweden. We build on this literature by introducing novel evidence on the effects of education on mental health in Africa, a context where this relationship has not yet been explored. Second, this paper adds to the vast literature exploring the effects of education on health, which largely builds on the model of health accumlation proposed by Grossman ( 1972 ) model of health accumulation. A recent review article finds that the effect of education on health outcomes (such as mortality and obesity) and health behaviors (such as smoking) is highly context specific (Galama et al., 2018 ). This implies that evidence from one context might not be applicable to others, especially if they vary significantly. Moreover, it is unclear a priori whether the relationship between education and health extends to mental health. Our paper adds to the growing literature on the link between education and health by bringing forth evidence on mental health, a novel and understudied outcome. 3
2. DATA AND KEY VARIABLES
The data used in this analysis comes from the World Health Survey (WHS). The WHS was conducted by the World Health Organization (WHO) across 70 countries between the years 2002 and 2004. The survey focused on topics related to health, and it aimed to generate detailed and synchronized information on population health and the state of health systems across the globe. We use data for Zimbabwe ‐ it was conducted in 2002 and sampled 4292 individuals across 4218 households. It is nationally representative, and the sample includes adults aged 18 years and above. Households were selected using a random, stratified sampling procedure, and one individual per household was selected for the interview. They also collected individual‐level information, including sociodemographic information, health state, health risk factors, chronic conditions, mortality, health care utilization, and social capital. We restrict our analysis to include people who were between the ages of zero and 30 in 1980, the year in which Zimbabwe implemented the education reform. This leaves us with a sample of 2604 individuals. Our analysis is based on the following self‐reported measures of mental health:
- Depression Index : This is based on the response to the following question: “Overall in the last 30 days, how much of a problem did you have with feeling sad, low or depressed?”. The responses are coded on a scale from one (“none”) to five (“extreme”).
- Any Depression Symptoms : This is a categorical variable that takes a value of one if the Depression Index takes a value greater than one.
- Anxiety Index : This is based on the response to the following question: “Overall in the last 30 days, how much of a problem did you have with worry or anxiety?”. The responses are coded on a scale from one (“none”) to five (“extreme”).
- Any Anxiety Symptoms : This is a categorical variable that takes a value of one if the Anxiety Index takes a value greater than one.
- Mean Index : This is a composite index created from the following measures: Depression Index, Anxiety Index, feeling depressed, 4 lost interest 5 and experiencing decreased energy. 6 For each covariate, we create a standardized measure (with zero mean and a standard deviation of one) and then average across these standardized measures to get this index.
The summary statistics corresponding to these measures are reported in Table 1 . The people in our sample have an average of around 8 years of education, and half of this sample has a secondary education. Around 70% of the individuals in our sample are male, and 60% live in rural areas. Nearly 40% of our sample reported suffering from some depression or anxiety‐related symptoms in the 30 days preceding the survey. The average severity of these reported symptoms in our sample are 1.8 for both depression and anxiety (measured on a scale ranging from one to five, where one is “none” and five is “extreme”).
Descriptive statistics
| Full sample | Ages 0–30 in 1980 | |||||
|---|---|---|---|---|---|---|
| Obs. | Mean | S.D. | Obs. | Mean | S.D. | |
| Years of education | 4063 | 7.5 | 4.0 | 2583 | 8.0 | 3.8 |
| Any secondary education (edu>7) | 4063 | 0.5 | 0.5 | 2583 | 0.5 | 0.5 |
| Age in 1980 (years) | 4089 | 14.3 | 16.2 | 2604 | 11.8 | 8.6 |
| Below 15 years in 1980 | 4100 | 0.6 | 0.5 | 2604 | 0.7 | 0.5 |
| Male (=1) | 4100 | 0.6 | 0.5 | 2604 | 0.7 | 0.5 |
| Rural (=1) | 4264 | 0.6 | 0.5 | 2588 | 0.6 | 0.5 |
| Mean index (Z‐score) | 4060 | −0.0 | 0.8 | 2588 | 0.0 | 0.8 |
| Depression index (1–5) | 4048 | 1.8 | 1.1 | 2580 | 1.8 | 1.1 |
| Any depression symptoms | 4048 | 0.4 | 0.5 | 2580 | 0.4 | 0.5 |
| Anxiety index (1–5) | 4044 | 1.8 | 1.1 | 2578 | 1.8 | 1.1 |
| Any anxiety symptoms | 4044 | 0.4 | 0.5 | 2578 | 0.4 | 0.5 |
Note : This is based on data from the World Health Survey for Zimbabwe.
3. ZIMBABWE EDUCATION REFORM: BACKGROUND
Zimbabwe declared its independence from the British rule in 1980. Under colonial rule, the education policy in Zimbabwe was designed to favor White students at the expense of Black students. The Ministry of Education had separate departments for White and Black students, with widely varying budgets and policies, which discriminated against the Black population. The government spent 12 times more per primary school pupil (grades 1–7) and three times more per secondary school pupil (grades 8–11) in the “European” system as opposed to the “Black” system. Primary schooling was free and compulsory for White students, while Black students had to pay fees and enrollment was voluntary. There were limited number of seats in secondary school for Black schoolchildren, and allocation was based on a competitive exam. This was in contrast to White students who gained automatic progression into secondary schools (Dorsey, 1989 ; Nhundu, 1989 , 1992 ).
After independence, the government implemented three key reforms aimed at equalizing educational opportunities for all – (1) government‐mandated free and compulsory primary schooling for all Zimbabweans, (2) automatic progression into secondary schools for everyone completing primary school (grades 1–7), and (3) the removal of age restrictions to allow over‐age children to enter school. To accommodate for the large demand for education, the government undertook a massive school building and reconstruction program. Between 1979 and 1981, the number of primary schools increased by 54%, while the number of secondary schools increased by 236% in the same period. The share of the budget allocated to education also increased from 11.6% in 1979–80 to 22.1% in 1980–81 (Nhundu, 1992 ). 7 More details on the changes in number of schools, teachers, and education expenditure that accompanied this policy are provided in Appendix A .
Overall, this resulted in sizable increases in enrollment into primary school (from around 800,000 in 1979 to 2.2 million in 1986) and secondary school (from 66,215 in 1979 to 537,427 in 1986). The larger proportional increase was experienced in secondary school enrollment because of the high levels of discrimination experienced in transition from primary to secondary schools in the pre‐reform period. Therefore, the policies targeted toward a smoother transition from primary to secondary school (removal of the mandatory exam) led to huge educational benefits for the Black population. This is also illustrated by the following statistic – the percentage of seventh graders who joined secondary school increased from 20% in 1979 to about 78% in 1986. This significant rise in the post‐reform period is demonstrated in Figure 1 – the plot shows that there was a large jump in the percentage of students who transitioned from primary to secondary school starting in the year 1980. This figure also shows that total secondary school enrollment, which had largely stayed constant before 1980, increased steadily in this period (Figure 1 ).

Trends in secondary school enrollment and transition for Zimbabwe. The estimates here are based on data from Riddell & Nyagura, 1991 , which in turn are curated from the UN statistical yearbooks from 1970 to 1988. The transition rate is the percentage of students who graduated from grade seven (highest grade in primary school) who end up enrolling in grade eight (secondary school). Secondary school enrollment is measured in thousands of students.
Put together, these reforms disproportionately benefited Black children who were in primary school (grades 1–7) at the time (and would have progressed to secondary school in the ensuing years). School starting age in Zimbabwe was 6 years – therefore, children aged 13 years and below at the time of the reform would have gained from the passage of this policy. In our main analysis, we consider this as our fully treated group. Since the reform also allowed for some overage children to enroll in school, there is the possibility that some 14 and 15 year old children could have also benefited due to the reforms – we consider them as partially treated. Those who were 16 years and above in 1980 were considerably less likely to have benefited from this policy change and hence form our control group.
4. EMPIRICAL METHODOLOGY
To explore the relationship between education and mental health, one would estimate the following specification:
where Y i is the mental health outcome for individual i , Education i is the education level of individual i , and X i includes gender, living in rural area, district and survey‐round fixed effects. OLS estimates of δ 1 , our coefficient of interest, would be biased because individuals with lower levels of education might also have other characteristics that could influence their mental health, such as lower income or worse physical health outcomes. To account for this bias, we use the exogenous shift in education caused by the Zimbabwean educational reform of 1980. As discussed earlier, this reform disproportionately increased access to education for Black children of primary school‐going age. Therefore, we create a categorical variable that divides our sample into a treated and a control group. Our treatment group consists of individuals who were 15 years or younger in 1980, and the control group consists of individuals who were 16 years or older at the same time. We implement a 2SLS‐IV framework, where the first stage equation uses the age‐specific exposure to the reform as an instrumental variable (IV) for years of education. In the second stage equation, we regress the outcome of interest on instrumented years of education. In this case, the equations of the first and second stage are as follows:
In Equation ( 3 ), β 1 represents the causal impact of education on long‐run mental health outcomes. Education i represents individual i 's education outcome, which in the main analysis will be years of education. In alternate specifications, we show that the results are robust to using a categorical variable for whether the individual had any secondary education (more than seventh grade). Treated i is a categorical variable that takes a value of one for individuals who were 15 years of age or below in 1980, and zero otherwise. The covariate f( Age80 i ‐15) accounts for different functional forms of age. In the main specifications we include linear polynomials, while in robustness checks we control for higher‐order polynomials (such as quadratic). This controls for any cohort‐specific effect on individuals born in a given year. 8
Standard errors are clustered at the level of the running variable, the age of the respondent in 1980. We control for gender, rural residence dummy, district fixed effects and temperature and rainfall shocks experienced by the individuals in their in‐utero period and infancy. The weather related controls are included to assuage concerns that these types of shocks experienced in childhood could be driving our findings (as shown by Adhvaryu et al., 2019 , who find that temperature shocks in the in‐utero period increase depressive symptoms in adulthood in Africa). The data for rainfall and temperature is at the district level and comes from the Willmott and Matsura series (Matsuura & Willmott, 2018 ). 9 In Appendix B , we further discuss the validity of this empirical strategy and present results from different checks, including McCrary density test (Figure A7 ) and falsification check related to effect on pre‐determined outcomes (Figure A8 ).
5.1. Impact of the 1980 reforms on educational attainment
We start by graphically examining the impact of the reform on educational attainment. To do this, we plot the highest grade attained ( y ‐axis) against age in the reform year ( x ‐axis). In Figure 2 we present graphs using the WHS data – the graph in the left panel demonstrates that years of education for the fully treated group (13 years and below) is considerably higher than that of the control group (16 years and above). The graph on the right in Figure 2 presents the same graph with the average years of education for 14 and 15 year olds (the partially treated group) included. The highest grade attained for the partially treated group is somewhere between the two aforementioned groups, confirming that some individuals of these cohorts benefited from the reforms. The same pattern is also observed using data from the Demographic and Health surveys 10 and 2012 Zimbabwe census data (Figure A2 ). Since the reform particularly focused on the transition from primary to secondary school, it is instructive to see if there had been a significant rise in the rate of secondary schooling among the treated group. We present the graphs pertaining to the share of the sample with secondary schooling in Figure A1 . The figure in the top panel suggests a discontinuous jump in the probability of attending secondary school among children aged 13 years and below, as compared to those who were 16 years or older at the time of the reform. Children who were 14 or 15 years of age again show a similar pattern as above (top panel, right graph). To demonstrate the robustness of the findings, we show that the effect of the reform is observed even when we use other datasets, the DHS (middle panel, Figure A1 ) and the 2012 census data (bottom panel, Figure A1 ).

Effects of the Reform on Education (First Stage effects). Authors' estimate based on Word Health Survey data. The y ‐axis represents the highest grade attained by individuals in our samples and the x ‐axis represents the age in 1980 when the reform was implemented. All estimations include gender, living in rural area, fixed effects for region and survey rounds. Standard errors are clustered by the age of respondent in 1980.
We further probe the effects of this reform on education by conducting regression analysis. In particular, in Table 2 , we present results corresponding to the first stage equation (Equation ( 2 )). In our analysis sample, treated individuals had on an average 3.4 additional years of schooling as compared to the untreated (Table 2 , column 1). This effect remains robust when restricting to smaller bandwidths around the age cutoff of 15 years (Table 2 , columns 2 and 3). The impact estimate remains statistically significant when we restrict the sample to individuals between 6 and 23 years of age (3.8 years, p ‐value < 0.001) and to those between 9 and 20 years of age (3.3 years, p ‐value < 0.001). The impact is larger and remains statistically significant among individuals living in rural areas (Table 2 , column 4). We present analogous results using any secondary education as an outcome in Table A3 ‐ the results follow a similar pattern to the findings above. The coefficient estimates of the impact of the reform on education presented here are larger in comparison to other studies in the same context. We posit that this is plausibly due to differences in the datasets used and the corresponding sample sizes in these analyses.
First stage ‐ effect of reform on years of education
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Variables | Full sample | 6–23 years | 9–20 years | Rural | Urban |
| Below 15 years in 1980 | 3.38*** | 3.78*** | 3.34*** | 3.51*** | 3.16*** |
| (0.18) | (0.47) | (1.09) | (0.23) | (0.34) | |
| Observations | 2442 | 1455 | 958 | 1551 | 891 |
| R‐squared | 0.35 | 0.31 | 0.28 | 0.28 | 0.30 |
| Mean ‐ full sample | 7.92 | 7.96 | 6.20 | 6.97 | 9.57 |
| Mean ‐ control | 5.62 | 6.17 | 6.17 | 4.93 | 7.36 |
| F‐stat (instrument) | 348 | 63 | 9 | 227 | 89 |
Note : Results are based on data from World Health Survey from Zimbabwe. The full sample includes individuals who were between the ages of 0 and 30 in 1980. All specifications exclude those who were 14 and 15 years old in 1980, and control for categorical variables for living in a rural area, fixed effects for survey round, and region and linear age trends, and rainfall/temperature shock in the year of birth. Standard errors are clustered by the age of the respondent in 1980.
* Significant at the 10 percent level. ** Significant at the 5 percent level. *** Significant at the 1 percent level.
We conduct two separate checks to demonstrate the robustness of the first stage effects. First, we use other datasets to show that the effect of the policy on education that we observe in the WHS dataset is present in other nationally representative surveys ‐ the Demographic and Health Surveys (Table A1 ) and the 2012 Census data (Table A2 ). We find a positive and statistically significant effect of the policy reform on education across different sub‐samples in both datasets. Additionally, we also show that the first stage effects are largely insensitive to changes in the bandwidth used ‐ in this check we restrict the sample of analysis to between 5 and 12 years on either side of the cutoff age and find that the reform's effect on education is preserved in the WHS data (Figure A3 ), the DHS data (top panel of Figure A4 ) and the 2012 census data (bottom panel of Figure A4 ).
5.2. Impact of education on mental health
Having established that the reform had a significant effect on educational outcomes, we explore whether this reform‐induced increase in education led to improved long‐run mental health. We first examine this using a graphical approach. In Figure 3 , we plot the distribution of mental health indices by treatment status. This figure illustrates that the treated group are more likely to report any symptoms related to anxiety/depression and are less likely to experience more severe symptoms related to anxiety/depression. This points toward the fact that the reform had a positive effect on mental health.

Values of mental health indices by treatment status. Based on Zimbabwe World Health Survey data. The figures plot the distribution of our measures of mental health: depression and anxiety indices, which measure the severity of symptoms related to depression and anxiety, in the top panels, and probability of having depression‐ or anxiety‐related symptoms in the bottom panels, by treatment status. Treated includes individuals aged 15 years and younger in 1980 and the untreated group consists of individuals aged 16 years and older in 1980.
Further, in Figure 4 , we present a plot of the impact of the reform on mental health. From this figure, we can conclude that the fully treated group (13 years and younger in 1980) is less likely to report symptoms related to anxiety or depression (Figure 4 , right) and have lower intensity symptoms related to depression and anxiety (Figure 4 , left).

The impact of education on mental health. Based on author calculations using World Health Survey Zimbabwe. The figures plot different measures of mental health against the running variable (age in 1980). The upper panels represent depression index (left) which measures the severity of the symptoms and an indicator variable for having any depression‐related symptoms (right). The lower panels presents graphs for similar outcomes pertaining to anxiety‐related symptoms.
As discussed in the empirical strategy section, the OLS specification (results in Table A4 ) will likely yield biased estimates of the impact of education on mental health due to the presence of other confounding factors such as income or physical health. Therefore, we conduct an IV analysis where years of education is instrumented using age‐based exposure to the Zimbabwean educational reform (based on Equations ( 2 ) and ( 3 )). These results are presented in Table 3 and suggest that an increase in education leads to better mental health, a consistent pattern across different mental health measures. Education decreases the probability of having any depression related symptoms by 11.3% (Table 3 , column 1) and those related to anxiety by 9.8% (Table 3 , column 2). 11 Additionally, education also reduces the severity of depressive symptoms by 6.1% (Table 3 , column 3) and anxiety by 5.6% (Table 3 , column 4). We also create a composite mental health index (combining the measures for depression and anxiety), where higher values indicate worse psychological health. We find that one more year of schooling leads to a decline in the composite mental health index by 0.06 standard deviations.
IV regressions – education and mental health
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Any depression | Any anxiety | Depression | Anxiety | Mean | |
| Variables | Symptoms | Symptoms | Index | Index | Index |
| Years of education | −0.06*** | −0.05*** | −0.12*** | −0.11*** | −0.06*** |
| (0.01) | (0.01) | (0.02) | (0.02) | (0.01) | |
| Observations | 2429 | 2427 | 2429 | 2427 | 2436 |
| Mean ‐ full sample | 0.45 | 0.44 | 1.80 | 1.80 | 0.00 |
| Mean ‐ control | 0.53 | 0.51 | 1.96 | 1.95 | 0.09 |
Note : Any Depression Symptoms and Any Anxiety Symptoms are categorical variables measuring whether the respondent suffered from any depressive or anxiety related symptoms. Depression Index and Anxiety index are measured on a scale of 1–5, where 5 represents more severe symptoms. The sample includes individuals who were between the ages of 0 and 30 in 1980. All specifications exclude those who were 14 and 15 years old in 1980, and control for categorical variables for living in a rural area, fixed effects for survey round, region and linear age trends, and rainfall/temperature shock in the year of birth. The control mean here refers to the mean of the outcome variable among those who were 16–30 years of age at the time of the reform. Results are based on data from World Health Survey from Zimbabwe. Standard errors are clustered by the age of the respondent in 1980.
* Significant at 10 percent. ** Significant at 5 percent. *** Significant at 1 percent.
Mechanisms – Physical health
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Self Rated | Diffulty | Any pain | Normal | |
| Variables | Health | Working | Or discomfort | BMI |
| Years of education | 0.05*** | −0.07*** | −0.06*** | 0.05*** |
| (0.01) | (0.01) | (0.01) | (0.01) | |
| Observations | 2442 | 2389 | 2442 | 1545 |
| Mean ‐ full sample | 0.19 | 0.39 | 0.50 | 0.59 |
| Mean ‐ control | 0.11 | 0.5 | 0.59 | 0.55 |
Note : The sample consists of individuals who were between 0 and 30 years of age in 1980 (excluding 14 and 15 year old). The control mean here refers to the mean of the outcome variable among those who were 16–30 years of age at the time of the reform. Standard errors are clustered by the age of the respondent in 1980.
Source : World Health Survey Zimbabwe.
Comparing the coefficient estimates from the OLS specifications (Table A4 ) with those from the IV specifications (Table 3 ) shows that the OLS estimates are underestimates of the true causal effect. This is consistent with other studies estimating the causal impact of education on health (Agüero & Bharadwaj, 2014 ; Cutler & Lleras‐Muney, 2010 ) and mental health specifically (Dursun & Cesur, 2016 ). The OLS could underestimate the true causal effect for a number of reasons. First, omitted variables (e.g., social norms such as gender roles) which might be negatively correlated with education might lead to a downward bias on the observed coefficient. Second, measurement error in education could lead to attenuation bias which would reduce the magnitude of the education coefficient. Third, IV estimates LATE, which is different from the average treatment effect estimated by OLS. The LATE is estimated based on compliers – this group consists of individuals who, in the absence of the reform, would not have had as much schooling, not because of any differences in their ability levels but because of higher‐than‐average costs of schooling due to the oppressive policies aimed at creating educational bottlenecks for the Black population. These are likely to be the more disadvantaged among the Black population, who in turn are likely to have worse mental health. Hence it is possible that these individuals demonstrate a higher marginal effect of education on mental health ‐ thus leading to the IV estimates being higher than the OLS.
Our results are akin to other studies that have found a positive impact of education on mental health in other contexts. For example, Crespo et al., 2014 find that an additional year of schooling decreases the probability of suffering from depression by 6.5% points. As another example, Dursun & Cesur, 2016 find that an increase of 3 years of schooling in Turkey increased life satisfaction among women by 0.17 standard deviation. Studies that look at the impact of early‐life shocks/interventions also find similar results. Analyzing a compulsory schooling reform in China that increased schooling among beneficiaries, Li & Sunder, 2022 find that an increase of one year of schooling leads to a decrease of 26% in the likelihood of being depressed and a 10% decline in the severity of depressive symptoms.
We would like to note two potential caveats to our study. In comparison to administrative data, survey respondents are less likely to report mental health problems due to social stigma (Bharadwaj et al., 2017 ; Greene et al., 2015 ). Therefore it is possible that the prevalence of mental illness observed in our data is less than the actual rates. Another concern is that the reporting of mental health could be correlated with educational attainment. A priori it is unclear what the direction of the association would be – one could argue that more educated individuals are more likely to under report mental health issues due to social stigma, while on the other hand lesser educated individuals might face societal pressures that increase their likelihood of reporting a mental illness. However, due to lack of evidence directly linking education with self‐reports of mental health, we are unable to provide a direction to this bias. 12
5.3. Heterogenous effects
Having established that an increase in education in childhood improves mental health later in life, we examine whether the relationship differs based on different socio‐economic characteristics.
First, we look at the impact of education on mental health by gender. Enrollment data shows that the Zimbabwean reform had a larger effect on girls ‐ the number of girls who enrolled in secondary school increased by tenfold between 1980 and 1985 (Chikuhwa, 2008 ). Therefore, we might expect that this increased educational effect might translate into larger positive impacts on women's mental health. Results in Figure 5 provide suggestive evidence supporting this ‐ education has a larger effect on mental health for women. One more year of education among women reduces the probability of having depression (14.8%) and anxiety (13%) related symptoms, while it also lowers the and the severity of these symptoms – depression (8.2%) and anxiety (7.1%). These effect sizes are larger than the overall effects, but the difference is not statistically significant. However, these results provide suggestive evidence of higher mental health gains among women. This gender‐differentiated impact is critical for two reasons. First, women have a higher prevalence of mood‐related disorders than men, possibly due to biological differences as well as lower self‐esteem, the experience of gender‐based violence, and gender discrimination (Boyd et al., 2015 ; Riecher‐Rössler, 2017 ). Our results suggest that education might mitigate some of these effects. Second, these mental health gains confer some intergenerational (indirect) benefits as well – studies have demonstrated that improved maternal mental health is associated with higher educational attainment, future household income, lower probability of criminal convictions (Johnston et al., 2013 ), and better health outcomes (Le & Nguyen, 2018 ). Since a majority of women in our sample are in the reproductive age range, improved mental health can not only improve their own well‐being, but also have strong implications for the long‐term human capital accumulation of the next generation as well.

Heterogeneous impacts of education on mental health. The definitions of the mental health measures are the same as those used in Table 3 . The sample includes women who were between the ages of 0 and 30 in 1980. All specifications exclude those who were 14 and 15 years old in 1980, and control for categorical variables for living in a rural area, fixed effects for survey round, region, linear age trends, and rainfall/temperature shock in the year of birth. Results are based on data from World Health Survey from Zimbabwe. Standard errors are clustered by the age of the respondent in 1980.
Next, we assess the impact of education on mental health among individuals living in rural areas. This is motivated by prior studies have found higher effects of educational reforms in rural areas (Erten & Keskin, 2018 ; Li & Sunder, 2022 ). In our case, the treated group in rural areas had 3.5 more years of education (Table 2 , column 4). This large increase in education in rural areas does translate into a higher positive impact on their mental health. Rural residents were seven p.p. and four p.p. less likely to report any symptoms related to depression and anxiety respectively in adulthood (Figure 5 ).
Finally, we examine whether individuals belonging to households with lower wealth experience any heterogeneous effects. In low‐ and middle‐income countries, low income is strongly associated with mental disorders (Rehm & Shield, 2019 ). Additionally, in developing country contexts, like Zimbabwe, the lower access to mental health resources and the inability of the poor to afford any available resources further adds to the problem. In this study, we measure assets using a composite asset index (created using principal component analysis 13 ) and define a household having low assets if it lies in or below the 25th percentile of the composite asset index distribution. Results in Figure 5 show that the impact of one additional year of schooling on mental health is indeed larger for this sub‐sample.
5.4. Robustness checks
We conduct several robustness checks to examine the sensitivity of our main empirical findings.
5.4.1. Bandwidth
We check whether our findings regarding the impact of education on mental health are robust to the use of different bandwidths around the age cutoff of 15 years. We replicate our main analysis using different bandwidths around the cutoff age – these bandwidths vary between 5 and 12 years, in 1‐year increments. The coefficient estimates from this exercise are presented in Figure A5 – they indicate that the effects of education on mental health are always negative (more education leads to better mental health) and largely remain statistically significant. This suggests that our main findings are largely insensitive to changes in bandwidth.
5.4.2. Polynomial function
In our main specification, we use a linear polynomial to control for the running variable, the age of the individual in 1980 minus 15. As a robustness check, we control for the running variable using a quadratic polynomial. The results presented in Figure A6 suggest that the impact of an extra year of education on all our measures of poor mental health remain negative and statistically significant.
5.4.3. Clustering of standard errors
We examine how sensitive our results are to clustering of the standard errors at different levels. In the main specification, standard errors are clustered by the age of the individual. But, there might be a high degree of correlation between the outcomes of people who live close to each other (in the same region), and hence including the region in the clustering may be desirable. Therefore, in Figure A6 we present results using two‐way clustering of the standard errors at the region‐age level. The results remain statistically significant.
5.4.4. Including partially treated individuals
As mentioned earlier, our main analysis excludes individuals who were 14 and 15 year old in 1980 (since they were partially treated the reform). Therefore, as a robustness check, we include them in the treated sample and re‐run our analysis. We find that the results remain similar in both size and statistical significance (Figure A6 ).
5.4.5. Changes in empirical strategy
Finally, we employ a slightly different empirical strategy than the one that is used in the main analysis (IV strategy). Here, we divide the treatment group into two separate categories – those who were completely treated, which includes individuals who were aged seven or below in 1980 (likely started primary school in/after 1980), and those who were partially treated, referring to people who were between 8 and 14 years of age in 1980 (likely to have already started primary school before the policy was implemented). The intuition behind creating these two groups is that individuals who were exposed to the policy throughout their primary schooling (completely treated) are likely to experience more benefits than those who were only benefited from it for a part of their primary schooling years (part treated). Results in Table A6 show that one more year of education among completely treated individuals led to a larger decrease in depression and anxiety symptoms, as well as the probability of reporting depression or anxiety symptoms compared to those who were only part treated, which is in line with our prior expectations.
5.5. Mechanisms
Further, we probe the potential mechanisms that might drive the observed effects of education on mental health in this context. Using various strands of medical, economic, and psychological literature, we explore several possible channels through which the mental health effects that we observe could have been mediated.
5.5.1. Physical health
Across a variety of contexts, it has been shown that physical health is strongly positively associated with mental health (Ohrnberger et al., 2017 ; Sabia & Rees, 2015 ; Willage, 2018 ). We examine whether improvements in education among the treated group in Zimbabwe led to improved physical health later in life. We measure physical health using the following indicators – self‐rated health (=1 if reported good health), whether the person had difficulty working in the past 30 days, whether they experienced any pain or discomfort in the last 30 days, and a categorical variable for whether their BMI was in the normal range (between 18.5 and 25). The results from this analysis are presented in Table 4 – they indicate that higher education led to better outcomes across all these indicators. More educated people reported better health (5 p.p.), experienced fewer difficulties/pain and had a five p.p. higher likelihood of having a BMI in the normal range. Additionally, they were seven p.p. and six p.p. less likely to report difficulty in working or any pain or discomfort, respectively. This implies that the Zimbabwean reform led to improved physical health outcomes, which in turn could be an important factor in driving the observed effects on mental health. 14
5.5.2. Health knowledge and behaviors
Past studies have demonstrated that improved health‐related practices (such as not smoking, lower alcohol consumption, and a healthy diet) are positively associated with mental well‐being (Buttery et al., 2015 ; Parletta et al., 2016 ). Therefore, we consider the following possibility: did educational gains among the treated cohorts also lead them to have improved health behaviors later in life, which in turn could have positively affected psychological health? In this analysis, we proxy health behaviors and knowledge using three different outcomes ‐ smoking/alcohol related behavior, HIV knowledge, 15 and knowledge/usage of various forms of contraception. With respect to smoking and alcohol consumption, we find that more educated individuals are less likely to be smoking (3 p.p.) or consuming alcohol (4 p.p.). The results in Table 5 also indicate a positive effect of schooling on enhanced knowledge of HIV among treated women – we find that women with higher education have more comprehensive knowledge about HIV (2 p.p.). Additionally, an increase in 1 year of education makes women five p.p. more likely to know about contraception 16 and increases their likelihood of using contraception by three p.p. (Table 5 , columns 4–5). Overall, this suggests that improved health‐related behaviors might be an important mediator of mental health gains.
Mechanisms – Health knowledge and behaviors
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| Any | Any | Comprehensive | Knows all | Ever used | |
| Variables | Alcohol | Smoking | HIV knowledge | Contraception | Contraception |
| Years of education | −0.04*** | −0.03*** | 0.02*** | 0.05*** | 0.03*** |
| (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | |
| Observations | 2416 | 2416 | 13,224 | 2856 | 13,224 |
| R‐squared | 0.19 | 0.15 | 0.31 | 0.01 | 0.56 |
| Mean ‐ full sample | 0.21 | 0.11 | 0.32 | 0.43 | 0.60 |
| Mean ‐ control | 0.28 | 0.16 | 0.22 | 0.38 | 0.69 |
Source : DHS Zimbabwe 1994, 1999, 2005.
5.5.3. Women's empowerment
There is growing evidence of a robust negative association between the prevalence of gender‐based violence and various measures of psychological challenges, including suicides, depression, post‐traumatic stress, and eating disorders (Grose et al., 2019 ). Using information from multiple rounds of the Zimbabwe DHS, we examine whether women's empowerment could have been a potential channel for the observed mental health effects. In particular, we explore the following three different dimensions of empowerment:
Mechanisms – Women's empowerment
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Number of | Sexual | Physical, sexual | Employed | |
| Variables | Decisions | Violence | & emotional violence | |
| Years of education | −0.00 | −0.02** | −0.01* | 0.03*** |
| (0.02) | (0.01) | (0.01) | (0.01) | |
| Observations | 6197 | 6269 | 6269 | 13,223 |
| Mean ‐ full sample | 1.72 | 0.10 | 0.06 | 0.48 |
| Mean ‐ control | 1.72 | 0.09 | 0.06 | 0.51 |
Note : Sexual violence is an indicator that takes the value of one if the woman experienced sexual violence from her partner in the last 12 months, and zero otherwise. Sexual & physical & emotional violence is an indicator that takes a value of one if the woman has ever experienced sexual, physical, and emotional violence from her partner, and zero otherwise. The sample consists of individuals who were between 0 and 30 years of age in 1980 (excluding 14 and 15 year old). The control mean here refers to the mean of the outcome variable among those who were 16–30 years of age at the time of the reform. Standard errors are clustered by the age of the respondent in 1980.
- Prevalence of IPV: Our findings suggest that women in the treated group have a 22 percent lower likelihood (relative to control mean) of reporting being the victim of sexual violence by their partners in the past 12 months. They are also less likely to have ever experienced physical and sexual, and emotional violence by their current partner (17 percent) (Table 6 , Columns 2 and 3).
Put together, these results point toward the role of increased empowerment among women, in the form of education‐induced reductions in IPV prevalence and increases in employment, as one of the potential mediators of the mental health benefits that we document.
6. DISCUSSION AND CONCLUSION
Mental health is a growing priority among policymakers, as indicated by its inclusion in the United Nations' Sustainable Goals (SDG). Despite the acknowledgment of its importance, investment in mental health has remained low, especially in Africa. 18 This has led to a shortfall in the availability of medicine, infrastructure, and health workers, which has resulted in large‐scale undertreatment of mental illness, the costs of which will become increasingly higher as the continent is expected to double its population in the next 3 decades (Sankoh et al., 2018 ). To the extent possible, our study examines whether, in contexts with limited health infrastructure, other complementary investments in childhood, such as education, could help decrease the burden of poor mental health in adulthood.
We study whether there is a causal link between education and mental health. We do so by leveraging the exogenous shift in education caused by a policy intervention in Zimbabwe. This reform removed significant barriers to education that Black schoolchildren in Zimbabwe faced and was effective in improving educational outcomes among the target population. Using nationally representative survey data and IV‐2SLS methodology, we find that an additional year of education reduces the probability of reporting any symptoms related to depression (11.3%) and anxiety (9.8%). Also, increased education has a dampening effect on the severity of symptoms related to both depression (6.1%) and anxiety (5.6%). Our results also indicate that the impact of education on mental health is larger for women and rural residents. In terms of mechanisms, we find that physical health, health knowledge (and behaviors) and women's empowerment might be crucial drivers of our findings.
This evidence on the protective effects of education on mental health is especially significant when viewed in conjunction with the mixed results demonstrated by other direct (and indirect) mental health‐enhancing interventions in similar contexts. For example, a review of the evidence on the relationship between poverty and depression and anxiety found that the average impact of anti‐poverty programs is a decrease in 0.094 SD in common mental health disorders such as depression and anxiety (0.138 SD for multi‐faceted anti‐poverty programs and 0.067 for cash transfer programs) (Ridley et al., 2020 ). These interventions are one‐off, potentially resource‐intensive, and affect only a small share of the population. In contrast, in this study, we show that large‐scale policy reform such as an expansion of education has a large and persistent long‐term impact on mental health, complementing similar evidence from other countries (Chevalier & Feinstein, 2006 ; Courtin et al., 2019 ; Crespo et al., 2014 ; Dursun & Cesur, 2016 ; Jiang et al., 2020 ; Lager et al., 2017 ; Mazzonna, 2014 ; Wang, 2021 ). These benefits become even more significant (and cost‐effective) since these education policies were not specifically designed to target these health outcomes and are spillover effects.
Our paper adds to the growing evidence on the efficacy of education in improving health outcomes in general (Galama et al., 2018 ) and to the understanding of the impact of interventions during adolescence on economic and social outcomes in adulthood (Cunha et al., 2010 ; Heckman, 2007 ). Our findings motivate future research on the impact of large‐scale policies in developing countries on understudied outcomes such as mental health, even if the interventions themselves were not directly targeted toward it.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
Supporting information
Supporting Information S1
Kondirolli, F. , & Sunder, N. (2022). Mental health effects of education . Health Economics , 31 ( S2 ), 22–39. 10.1002/hec.4565 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
1 Using multiple data sources (including census data), we demonstrate in our analysis that those who were 16 years or older had a much lower likelihood of experiencing educational gains due to this policy. This pattern has also been confirmed by other studies of the same policy intervention (Agüero & Ramachandran, 2020 ; Grépin & Bharadwaj, 2015 ).
2 Broadly, economic research on mental health has largely focused on developed countries, and has examined different determinants of mental well‐being, such as income (Baird et al., 2013 ; Haushofer & Shapiro, 2016 ; Kahneman & Deaton, 2010 ; Kahneman & Krueger, 2006 ; Stevenson & Wolfers, 2013 ), poverty (Haushofer & Fehr, 2014 ; Lund et al., 2011 ; Tsaneva & Balakrishnan, 2019 ), environment (Zhang et al., 2017 ), socioeconomic status (Lorant et al., 2003 ; Stewart‐Brown et al., 2015 ), crime (Bor et al., 2018 ; Cornaglia et al., 2014 ; Dustmann & Fasani, 2016 ; Metcalfe et al., 2011 ), early‐life circumstances (Adhvaryu et al., 2019 ; Dinkelman, 2017 ; Persson & Rossin‐Slater, 2018 ), career choices (Bertrand, 2013 ), residential status (Katz et al., 2001 ), and migration (Scheffel & Zhang, 2019 ).
3 Other papers that have looked at the effect of education on health (and related) outcomes in the African context include child mortality (Grépin & Bharadwaj, 2015 ; Keats, 2018 ), fertility (Osili & Long, 2008 ), HIV prevalence (Duflo et al., 2015 ), and teenage pregnancy (Baird et al., 2013 ).
4 Takes a value of one if the response to the following question is “Yes” (and zero otherwise): “During the last 12 months, have you had a period lasting several days when you felt sad, empty or depressed?”
5 Takes a value of one if the response to the following question is “Yes” (and zero otherwise): “During the last 12 months, have you had a period lasting several days when you lost interest in most things you usually enjoy such as hobbies, personal relationships or work?”
6 Takes a value of one if the response to the following question is “Yes” (and zero otherwise): “During the last 12 months, have you had a period lasting several days when you have been feeling your energy decreased or that you are tired all the time?”
7 The demand for education could not be met with a proportional increase in the supply of teachers in years immediately after 1980, which possibly led to the government hiring untrained and under‐qualified teachers (according to some sources the share of untrained teachers was as high as 43 percent in 1987 (Nhundu, 1992 )). To increase the supply of trained teachers, the University of Zimbabwe offered a 2‐year part‐time course for teachers who were already working in secondary schools and the government introduced the Zimbabwe Integrated National Teacher Education Course, that consisted of an one‐term teaching course followed by a three and half years of teaching in primary (and subsequently secondary) schools.
8 Any differences between the treatment and control cohorts due to factors not controlled for in our specification would be a concern if they were to differentially affect those that are just below and those just above the cutoff age – which we think this is unlikely to be the case. Having said that, we note this as a caveat of this analysis. Additionally, we do not know of any other policies or reforms implemented concurrently in Zimbabwe that was targeted in the same manner as this education reform.
9 Rainfall and temperature shocks are defined using the following formula: log(average over a given 12 month period) minus log(long term mean).
10 We use the 1994, 1999, and 2005 rounds of the Demographic and Health surveys in Zimbabwe.
11 The effect sizes are relative to control group mean. Since the reform targeted entry into secondary school, in an alternate specification we use a categorical variable for having any secondary education as the main independent variable of interest (instead of years of education). As expected, having any secondary education has a large positive impact on mental health (estimates in Table A5 ).
12 Some studies show that people with more education are less likely to self‐report being sick (Subramanian et al., 2009 ) and have a lower likelihood of reporting worse health status (Subramanian et al., 2010 ). Using WHS data, Subramanian et al., 2010 show that this pattern is observed across countries with different income status. This indicates that more educated people are less likely to report worse health, and there is a possibility that a similar pattern may exist for mental health as well.
13 This composite asset index is based on household ownership of the following items – bicycle, clock, bucket, washing machine, refrigerator, telephone, mobile phone, television, computer, wheel‐barrow, cart and radio. Note that the wealth heterogeneity results should be interpreted with the caveat that we are stratifying on a post‐treatment (endogenous) variable.
14 It is to be noted that the mechanisms analysis presented here is suggestive in nature, and that a bulk of the outcomes examined here are measured contemporaneously with the mental health measure.
15 We use HIV because Zimbabwe has the fifth highest prevalence of HIV in the world with, 12.8 percent of the population aged 15–49 years old infected (The World Bank, 2015 ). Here, comprehensive knowledge of HIV is a categorical variable that takes the value of one if an individual knows that they can reduce HIV risk by limiting the number of partners and using condoms, that a healthy person can have HIV, that HIV cannot be transmitted by mosquito bites or supernatural means, and zero otherwise. These findings are consistent with those of Agüero and Bharadwaj ( 2014 ).
16 These methods of contraception include female sterilization, male sterilization, pill, IUD, injectables, implants, male condoms, female condom, diaphragm, standard days method, LAM, emergency contraception, rhythm method, and withdrawal method.
17 These decision‐making categories include the following: her own health, large household purchases and visiting friends/family. We create a categorical variable for each of these, where it takes a value of one if the woman is involved in the decision (either deciding by herself or jointly with the husband). We also create an additional composite variable on whether the woman is involved in making all of the above decisions – this takes a value of one if she is involved in all of the decisions, and zero otherwise; and a variable that represents the number of decisions she is involved in.
18 In 2017 the median per‐capita mental health expenditure in Africa was 10 cents, as compared to a global average of USD 2.5 (WHO, 2018 ). This has led to low levels of health personnel (per‐capita median number of mental health workers in Africa is 1/50th that of Europe), and admission rates to mental health institutions (0.2 per 1000 population as compared to 4.5 per 1000 population in Europe).
DATA AVAILABILITY STATEMENT
- Adhvaryu, A. , Fenske, J. , & Nyshadham, A. (2019). Early life circumstance and adult mental health . Journal of Political Economy , 127 ( 4 ), 1516–1549. 10.1086/701606 [ CrossRef ] [ Google Scholar ]
- Agüero, J. M. , & Bharadwaj, P. (2014). Do the more educated know more about health? Evidence from schooling and HIV knowledge in Zimbabwe . Economic Development and Cultural Change , 62 ( 3 ), 489–517. 10.1086/675398 [ CrossRef ] [ Google Scholar ]
- Agüero, J. M. , & Ramachandran, M. (2020). The intergenerational transmission of schooling among the education‐rationed . Journal of Human Resources , 55 ( 2 ), 504–538. 10.3368/jhr.55.2.0816.8143r [ CrossRef ] [ Google Scholar ]
- Anderberg, D. , Rainer, H. , Wadsworth, J. , & Wilson, T. (2016). Unemployment and domestic violence: Theory and evidence . Economic Journal , 126 ( 597 ), 1947–1979. 10.1111/ecoj.12246 [ CrossRef ] [ Google Scholar ]
- Avendano, M. , de Coulon, A. , & Nafilyan, V. (2020). Does longer compulsory schooling affect mental health? Evidence from a British reform . Journal of Public Economics , 183 , 104137. 10.1016/j.jpubeco.2020.104137 [ CrossRef ] [ Google Scholar ]
- Baird, S. , de Hoop, J. , & Özler, B. (2013). Income shocks and adolescent mental health . Journal of Human Resources , 48 ( 2 ), 370–403. 10.1353/jhr.2013.0014 [ CrossRef ] [ Google Scholar ]
- Begerow, T. , & Jürges, H. (2021). Does compulsory schooling affect health? Evidence from ambulatory claims data . The European Journal of Health Economics , 1 , 1–16. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Bertrand, M. (2013). Career, family, and the well‐being of college‐educated women . The American Economic Review , 103 ( 3 ), 244–250. 10.1257/aer.103.3.244 [ CrossRef ] [ Google Scholar ]
- Bharadwaj, P. , Pai, M. M. , & Suziedelyte, A. (2017). Mental health stigma . Economics Letters , 159 , 57–60. 10.1016/j.econlet.2017.06.028 [ CrossRef ] [ Google Scholar ]
- Bloom, D. E. , Cafiero, E. , Jané‐Llopis, E. , Abrahams‐Gessel, S. , Bloom, L. R. , Fathima, S. , Feigl, A. B. , Gaziano, T. , Hamandi, A. , Mowafi, M. , Pandya, A. , Prettner, K. , Rosenberg, L. , Seligman, B. , Stein, A. Z. , & Weinstein, C. (2011). The global economic burden of noncommunicable diseases . World Economic Forum. [ Google Scholar ]
- Böckerman, P. , Haapanen, M. , Jepsen, C. , & Roulet, A. (2021). School tracking and mental health . Journal of Human Capital , 15 ( 2 ), 291–345. 10.1086/712728 [ CrossRef ] [ Google Scholar ]
- Bor, J. , Venkataramani, A. S. , Williams, D. R. , & Tsai, A. C. (2018). Police killings and their spillover effects on the mental health of black Americans: A population‐based, quasi‐experimental study . The Lancet , 392 ( 10144 ), 302–310. 10.1016/s0140-6736(18)31130-9 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Boyd, A. , Van De Velde, S. , Vilagut, G. , De Graaf, R. , O’Neill, S. , Florescu, S. , Alonso, J. , & Kovess‐Masfety, V. (2015). Gender differences in mental disorders and suicidality in Europe: Results from a large cross‐sectional population‐based study . Journal of Affective Disorders , 173 , 245–254. 10.1016/j.jad.2014.11.002 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Buttery, A. K. , Mensink, G. B. , & Busch, M. A. (2015). Healthy behaviours and mental health: Findings from the German health update (GEDA) . The European Journal of Public Health , 25 ( 2 ), 219–225. 10.1093/eurpub/cku094 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Chevalier, A. , & Feinstein, L. (2006). Sheepskin or prozac: The causal effect of education on mental health . SSRN Electronic Journal . 10.2139/ssrn.923530 [ CrossRef ] [ Google Scholar ]
- Chikuhwa, J. (2008). Zimbabwe: Beyond a school certificate .
- Cornaglia, F. , Feldman, N. E. , & Leigh, A. (2014). Crime and mental well‐being . Journal of Human Resources , 49 ( 1 ), 110–140. 10.1353/jhr.2014.0005 [ CrossRef ] [ Google Scholar ]
- Courtin, E. , Nafilyan, V. , Glymour, M. , Goldberg, M. , Berr, C. , Berkman, L. F. , Zins, M. , & Avendano, M. (2019). Long‐term effects of compulsory schooling on physical, mental and cognitive ageing: A natural experiment . Journal of Epidemiology & Community Health , 73 ( 4 ), 370–376. 10.1136/jech-2018-211746 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Crespo, L. , López‐Noval, B. , & Mira, P. (2014). Compulsory schooling, education, depression and memory: New evidence from SHARELIFE . Economics of Education Review , 43 , 36–46. 10.1016/j.econedurev.2014.09.003 [ CrossRef ] [ Google Scholar ]
- Cunha, F. , Heckman, J. J. , Schennach, S. M. , Attanasio, O. , Becker, G. , Cattan, S. , Eisenhauer, P. , Gen‐Sowski, M. , Grogger, J. , Hansen, L. , Hansman, C. , Murphy, K. , Todd, P. , Williams, B. , Wolpin, K. , Yi, J. , Cunha, F. , Heckman, J. J. , & Schennach, S. M. (2010). Estimating the technology of cognitive and noncognitive skill formation . Econometrica , 78 ( 3 ), 883–931. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Cutler, D. M. , & Lleras‐Muney, A. (2010). Understanding differences in health behaviors by education . Journal of Health Economics , 29 ( 1 ), 1–28. 10.1016/j.jhealeco.2009.10.003 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Dinkelman, T. (2017). Long‐run health repercussions of drought shocks: Evidence from South African homelands . Economic Journal , 127 ( 604 ), 1906–1939. 10.1111/ecoj.12361 [ CrossRef ] [ Google Scholar ]
- Dorsey, B. J. (1989). Educational development and reform in Zimbabwe . Comparative Education Review , 33 ( 1 ), 40–58. 10.1086/446811 [ CrossRef ] [ Google Scholar ]
- Duflo, E. , Dupas, P. , & Kremer, M. (2015). Education, HIV, and early fertility: Experimental evidence from Kenya . The American Economic Review , 105 ( 9 ), 2757–2797. 10.1257/aer.20121607 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Dursun, B. , & Cesur, R. (2016). Transforming lives: The impact of compulsory schooling on hope and happiness . Journal of Population Economics , 29 ( 3 ), 911–956. 10.1007/s00148-016-0592-1 [ CrossRef ] [ Google Scholar ]
- Dustmann, C. , & Fasani, F. (2016). The effect of local area crime on mental health . Economic Journal , 126 ( 593 ), 978–1017. 10.1111/ecoj.12205 [ CrossRef ] [ Google Scholar ]
- Erten, B. , & Keskin, P. (2018). For better or for worse? Education and the prevalence of domestic violence in Turkey . American Economic Journal: Applied Economics , 10 ( 1 ), 64–105. 10.1257/app.20160278 [ CrossRef ] [ Google Scholar ]
- Frijters, P. , Johnston, D. W. , & Shields, M. A. (2014). The effect of mental health on employment: Evidence from Australian panel data . Health Economics , 23 ( 9 ), 1058–1071. 10.1002/hec.3083 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Galama, T. J. , van Kippersluis, H. , & Lleras‐Muney, A. (2018). The effect of education on health and mortality: A review of experimental and quasi‐experimental evidence . National Bureau of Economic Research , 53 ( 9 ), 287. [ Google Scholar ]
- Graham, C. , Eggers, A. , & Sukhtankar, S. (2004). Does happiness pay? An exploration based on panel data from Russia . Journal of Economic Behavior & Organization , 55 ( 3 ), 319–342. 10.1016/s0167-2681(04)00047-2 [ CrossRef ] [ Google Scholar ]
- Graham, C. , & Pinto, S. (2019). Unequal hopes and lives in the USA: Optimism, race, place, and premature mortality . Journal of Population Economics , 32 ( 2 ), 665–733. 10.1007/s00148-018-0687-y [ CrossRef ] [ Google Scholar ]
- Greene, W. H. , Harris, M. N. , & Hollingsworth, B. (2015). Inflated responses in measures of self‐assessed health . American Journal of Health Economics , 1 ( 4 ), 461–493. 10.1162/ajhe_a_00026 [ CrossRef ] [ Google Scholar ]
- Grépin, K. A. , & Bharadwaj, P. (2015). Maternal education and child mortality in Zimbabwe . Journal of Health Economics , 44 , 97–117. 10.1016/j.jhealeco.2015.08.003 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Grose, R. G. , Roof, K. A. , Semenza, D. C. , Leroux, X. , & Yount, K. M. (2019). Mental health, empowerment, and violence against young women in lower‐income countries: A review of reviews . Aggression and Violent Behavior , 46 , 25–36. 10.1016/j.avb.2019.01.007 [ CrossRef ] [ Google Scholar ]
- Grossman, M. (1972). On the concept of health capital and the demand for health . Journal of Political Economy , 80 ( 2 ), 223–255. 10.1086/259880 [ CrossRef ] [ Google Scholar ]
- Haushofer, J. , & Fehr, E. (2014). On the psychology of poverty . Science , 344 ( 6186 ), 862–867. 10.1126/science.1232491 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Haushofer, J. , & Shapiro, J. (2016). The short‐term impact of unconditional cash transfers to the poor: Experimental evidence from Kenya . Quarterly Journal of Economics , 131 ( 4 ), 1973–2042. 10.1093/qje/qjw025 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Heckman, J. J. (2007). The economics, technology, and neuroscience of human capability formation . Proceedings of the National Academy of Sciences of the United States of America , 104 ( 33 ), 13250–13255. 10.1073/pnas.0701362104 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Hobkirk, A. L. , Towe, S. L. , Lion, R. , & Meade, C. S. (2015). Primary and secondary HIV prevention among persons with severe mental illness: Recent findings . Current HIV , 12 ( 4 ), 406–412. 10.1007/s11904-015-0294-4 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- James, S. L. (2018). Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990‐2017: A systematic analysis for the global burden of disease study 2017 . The Lancet , 392 ( 10159 ), 1789–1858. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Jiang, W. , Lu, Y. , & Xie, H. (2020). Education and mental health: Evidence and mechanisms . Journal of Economic Behavior & Organization , 180 , 407–437. 10.1016/j.jebo.2020.09.032 [ CrossRef ] [ Google Scholar ]
- Johnston, D. W. , Schurer, S. , & Shields, M. A. (2013). Exploring the intergenerational persistence of mental health: Evidence from three generations . Journal of Health Economics , 32 ( 6 ), 1077–1089. 10.1016/j.jhealeco.2013.09.001 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kahneman, D. , & Deaton, A. (2010). High income improves evaluation of life but not emotional well‐being . Proceedings of the National Academy of Sciences of the United States of America , 107 ( 38 ), 16489–16493. 10.1073/pnas.1011492107 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kahneman, D. , & Krueger, A. B. (2006). Developments in the measurement of subjective well‐being . The Journal of Economic Perspectives , 20 ( 1 ), 3–24. 10.1257/089533006776526030 [ CrossRef ] [ Google Scholar ]
- Katz, L. F. , Kling, J. R. , & Liebman, J. B. (2001). Moving to opportunity in Boston: Early results of a randomized mobility experiment . Quarterly Journal of Economics , 116 ( 2 ), 607–654. 10.1162/00335530151144113 [ CrossRef ] [ Google Scholar ]
- Keats, A. (2018). Women’s schooling, fertility, and child health outcomes: Evidence from Uganda’s free primary education program . Journal of Development Economics , 135 , 142–159. 10.1016/j.jdeveco.2018.07.002 [ CrossRef ] [ Google Scholar ]
- Koschorke, M. , Padmavati, R. , Kumar, S. , Cohen, A. , Weiss, H. A. , Chatterjee, S. , Pereira, J. , Naik, S. , John, S. , Dabholkar, H. , Balaji, M. , Chavan, A. , Varghese, M. , Thara, R. , Thornicroft, G. , & Patel, V. (2014). Experiences of stigma and discrimination of people with schizophrenia in India . Social science medicine (1982) , 123 , 149–159. 10.1016/j.socscimed.2014.10.035 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Lager, A. , Seblova, D. , Falkstedt, D. , & Lövdén, M. (2017). Cognitive and emotional outcomes after prolonged education: A quasi‐experiment on 320 182 Swedish boys . International Journal of Epidemiology , 46 ( 1 ), 303–311. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Le, H. T. , & Nguyen, H. T. (2018). The impact of maternal mental health shocks on child health: Estimates from fixed‐effects instrumental variables models for two cohorts of Australian children . American Journal of Health Economics , 4 ( 2 ), 185–225. 10.1162/ajhe_a_00100 [ CrossRef ] [ Google Scholar ]
- Li, Y. and Sunder, N. (2022). Education and mental health: Evidence from China . Working Paper.
- Lorant, V. , Deliège, D. , Eaton, W. , Robert, A. , Philippot, P. , & Ansseau, M. (2003). Socioeconomic inequalities in depression: A meta‐analysis . American Journal of Epidemiology , 157 ( 2 ), 98–112. 10.1093/aje/kwf182 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Lund, C. , De Silva, M. , Plagerson, S. , Cooper, S. , Chisholm, D. , Das, J. , Knapp, M. , & Patel, V. (2011). Poverty and mental disorders: Breaking the cycle in low‐income and middle‐income countries . The Lancet , 378 ( 9801 ), 1502–1514. 10.1016/s0140-6736(11)60754-x [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Majlesi, K. (2016). Labor market opportunities and women’s decision making power within households . Journal of Development Economics , 119 , 34–47. 10.1016/j.jdeveco.2015.10.002 [ CrossRef ] [ Google Scholar ]
- Mascayano, F. , Armijo, J. E. , & Yang, L. H. (2015). Addressing stigma relating to mental illness in low‐ and middle‐income countries . Frontiers in Psychiatry , 6 . 10.3389/fpsyt.2015.00038 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Matsuura, K. , & Willmott, C. (2018). Willmott, Matsuura and collaborators climate resource .
- Mazzonna, F. (2014). The long lasting effects of education on old age health: Evidence of gender differences . Social Science & Medicine , 101 , 129–138. 10.1016/j.socscimed.2013.10.042 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Metcalfe, R. , Powdthavee, N. , & Dolan, P. (2011). Destruction and distress: Using a quasi‐experiment to show the effects of the September 11 attacks on mental well‐being in the United Kingdom . Economic Journal , 121 ( 550 ), 81–F103. 10.1111/j.1468-0297.2010.02416.x [ CrossRef ] [ Google Scholar ]
- Nhundu, T. J. (1989). The financing and provision of education in Zimbabwe: Towards greater equality? Educational Review , 41 ( 3 ), 243–253. 10.1080/0013191890410304 [ CrossRef ] [ Google Scholar ]
- Nhundu, T. J. (1992). A decade of educational expansion in Zimbabwe: Causes, consequences, and policy Ccntradictions . The Journal of Negro Education , 61 ( 1 ), 78. 10.2307/2295630 [ CrossRef ] [ Google Scholar ]
- Ohrnberger, J. , Fichera, E. , & Sutton, M. (2017). The relationship between physical and mental health: A mediation analysis . Social Science & Medicine , 195 , 42–49. 10.1016/j.socscimed.2017.11.008 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Oshodi, Y. O. , Abdulmalik, J. , Ola, B. , James, B. O. , Bonetto, C. , Cristofalo, D. , Bortel, T. V. , Sartorius, N. , & Thornicroft, G. (2014). Pattern of experienced and anticipated discrimination among people with depression in Nigeria: A cross‐sectional study . Social Psychiatry and Psychiatric Epidemiology , 49 ( 2 ), 259–266. 10.1007/s00127-013-0737-4 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Osili, U. O. , & Long, B. T. (2008). Does female schooling reduce fertility? Evidence from Nigeria . Journal of Development Economics , 87 ( 1 ), 57–75. 10.1016/j.jdeveco.2007.10.003 [ CrossRef ] [ Google Scholar ]
- Oswald, A. J. , Proto, E. , & Sgroi, D. (2015). Happiness and productivity . Journal of Labor Economics , 33 ( 4 ), 789–822. 10.1086/681096 [ CrossRef ] [ Google Scholar ]
- Parletta, N. , Aljeesh, Y. , & Baune, B. T. (2016). Health behaviors, knowledge, life satisfaction, and wellbeing in people with mental illness across four countries and comparisons with normative sample . Frontiers in Psychiatry , 7 ( AUG ), 22. 10.3389/fpsyt.2016.00145 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Patel, V. , Maj, M. , Flisher, A. J. , De Silva, M. J. , Koschorke, M. , Prince, M. , Zonal, W. P. A. , Riba, M. , Sanchez, M. , Campodonico, F. D. , Risco, L. , Gask, L. , Wahlberg, H. , Roca, M. , Lecic‐Tosevski, D. , Soghoyan, A. , Moussaoui, D. , Baddoura, C. , Adeyemi, J. , …, & Richardson, G. (2010). Reducing the treatment gap for mental disorders: A WPA survey . World Psychiatry , 9 ( 3 ), 169–176. 10.1002/j.2051-5545.2010.tb00305.x [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Persson, P. , & Rossin‐Slater, M. (2018). Family ruptures, stress, and the mental health of the next generation . The American Economic Review , 108 ( 4–5 ), 1214–1252. 10.1257/aer.20141406 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Prince, M. , Patel, V. , Saxena, S. , Maj, M. , Maselko, J. , Phillips, M. R. , & Rahman, A. (2007). No health without mental health . Lancet , 370 ( 9590 ), 859–877. 10.1016/s0140-6736(07)61238-0 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Rehm, J. , & Shield, K. D. (2019). Global burden of disease and the impact of mental and addictive disorders . Current Psychiatry Reports , 21 ( 2 ), 10. 10.1007/s11920-019-0997-0 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Riddell, A. R. , & Nyagura, L. M. (1991). What causes differences in achievement in Zimbabwe’s secondary schools? Population and Human Resources Department, World Bank. [ Google Scholar ]
- Ridley, M. , Rao, G. , Schilbach, F. , & Patel, V. (2020). Poverty, depression, and anxiety: Causal evidence and mechanisms . Science , 370 ( 6522 ). 10.1126/science.aay0214 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Riecher‐Rössler, A. (2017). Sex and gender differences in mental disorders . The Lancet Psychiatry , 4 ( 1 ), 8–9. 10.1016/s2215-0366(16)30348-0 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Sabia, J. J. , & Rees, D. I. (2015). Body weight, mental health capital, and academic achievement . Review of Economics of the Household , 13 ( 3 ), 653–684. 10.1007/s11150-014-9272-7 [ CrossRef ] [ Google Scholar ]
- Sankoh, O. , Sevalie, S. , & Weston, M. (2018). Mental health in Africa . Lancet Global Health , 6 ( 9 ), e954–e955. 10.1016/s2214-109x(18)30303-6 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Scheffel, J. , & Zhang, Y. (2019). How does internal migration affect the emotional health of elderly parents left‐behind? Journal of Population Economics , 32 ( 3 ), 953–980. 10.1007/s00148-018-0715-y [ CrossRef ] [ Google Scholar ]
- Shibre, T. , Negash, A. , Kullgren, G. , Kebede, D. , Alem, A. , Fekadu, A. , Fekadu, D. , Medhin, G. , & Jacobsson, L. (2001). Perception of stigma among family members of individuals with schizophrenia and major affective disorders in rural Ethiopia . Social Psychiatry and Psychiatric Epidemiology , 36 ( 6 ), 299–303. 10.1007/s001270170048 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Stevenson, B. , & Wolfers, J. (2013). Subjective well‐being and income: Is there any evidence of satiation? The American Economic Review , 103 ( 3 ), 598–604. 10.1257/aer.103.3.598 [ CrossRef ] [ Google Scholar ]
- Stewart‐Brown, S. , Samaraweera, P. C. , Taggart, F. , Kandala, N. B. , & Stranges, S. (2015). Socioeconomic gradients and mental health: Implications for public health . British Journal of Psychiatry , 206 ( 6 ), 461–465. 10.1192/bjp.bp.114.147280 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Subramanian, S. V. , Huijts, T. , & Avendano, M. (2010). Self‐reported health assessments in the 2002 world health survey: How do they correlate with education? Bulletin of the World Health Organization , 88 ( 2 ), 131–138. 10.2471/blt.08.067058 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Subramanian, S. V. , Subramanyam, M. A. , Selvaraj, S. , & Kawachi, I. (2009). Are self‐reports of health and morbidities in developing countries misleading? Evidence from India . Social Science & Medicine . [ PMC free article ] [ PubMed ] [ Google Scholar ]
- The World Bank . (2015). Prevalence of HIV, total . (% of population ages 15‐49).
- Tsaneva, M. , & Balakrishnan, U. (2019). The effect of a Workfare programme on psychological wellbeing in India . Journal of Development Studies , 55 ( 12 ), 2593–2609. 10.1080/00220388.2018.1502879 [ CrossRef ] [ Google Scholar ]
- Wahlbeck, K. , Westman, J. , Nordentoft, M. , Gissler, M. , & Laursen, T. M. (2011). Outcomes of Nordic mental health systems: Life expectancy of patients with mental disorders . British Journal of Psychiatry , 199 ( 6 ), 453–458. 10.1192/bjp.bp.110.085100 [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Wang, T. (2021). The impact of education on mental health: Evidence from compulsory education law in China . 10.1080/13504851.2021.1946002 [ CrossRef ]
- WHO . (2018). Mental health atlas 2017 .
- Willage, B. (2018). The effect of weight on mental health: New evidence using genetic IVs . Journal of Health Economics , 57 , 113–130. 10.1016/j.jhealeco.2017.11.003 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Zhang, X. , Zhang, X. , & Chen, X. (2017). Happiness in the air: How does a dirty sky affect mental health and subjective well‐being? Journal of Environmental Economics and Management , 85 , 81–94. 10.1016/j.jeem.2017.04.001 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Future Students
- Current Students
- Faculty/Staff
News and Media
- News & Media Home
- Research Stories
- School’s In
- In the Media
You are here
More than two hours of homework may be counterproductive, research suggests.
")
A Stanford education researcher found that too much homework can negatively affect kids, especially their lives away from school, where family, friends and activities matter. "Our findings on the effects of homework challenge the traditional assumption that homework is inherently good," wrote Denise Pope , a senior lecturer at the Stanford Graduate School of Education and a co-author of a study published in the Journal of Experimental Education . The researchers used survey data to examine perceptions about homework, student well-being and behavioral engagement in a sample of 4,317 students from 10 high-performing high schools in upper-middle-class California communities. Along with the survey data, Pope and her colleagues used open-ended answers to explore the students' views on homework. Median household income exceeded $90,000 in these communities, and 93 percent of the students went on to college, either two-year or four-year. Students in these schools average about 3.1 hours of homework each night. "The findings address how current homework practices in privileged, high-performing schools sustain students' advantage in competitive climates yet hinder learning, full engagement and well-being," Pope wrote. Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school. Their study found that too much homework is associated with: • Greater stress : 56 percent of the students considered homework a primary source of stress, according to the survey data. Forty-three percent viewed tests as a primary stressor, while 33 percent put the pressure to get good grades in that category. Less than 1 percent of the students said homework was not a stressor. • Reductions in health : In their open-ended answers, many students said their homework load led to sleep deprivation and other health problems. The researchers asked students whether they experienced health issues such as headaches, exhaustion, sleep deprivation, weight loss and stomach problems. • Less time for friends, family and extracurricular pursuits : Both the survey data and student responses indicate that spending too much time on homework meant that students were "not meeting their developmental needs or cultivating other critical life skills," according to the researchers. Students were more likely to drop activities, not see friends or family, and not pursue hobbies they enjoy. A balancing act The results offer empirical evidence that many students struggle to find balance between homework, extracurricular activities and social time, the researchers said. Many students felt forced or obligated to choose homework over developing other talents or skills. Also, there was no relationship between the time spent on homework and how much the student enjoyed it. The research quoted students as saying they often do homework they see as "pointless" or "mindless" in order to keep their grades up. "This kind of busy work, by its very nature, discourages learning and instead promotes doing homework simply to get points," said Pope, who is also a co-founder of Challenge Success , a nonprofit organization affiliated with the GSE that conducts research and works with schools and parents to improve students' educational experiences.. Pope said the research calls into question the value of assigning large amounts of homework in high-performing schools. Homework should not be simply assigned as a routine practice, she said. "Rather, any homework assigned should have a purpose and benefit, and it should be designed to cultivate learning and development," wrote Pope. High-performing paradox In places where students attend high-performing schools, too much homework can reduce their time to foster skills in the area of personal responsibility, the researchers concluded. "Young people are spending more time alone," they wrote, "which means less time for family and fewer opportunities to engage in their communities." Student perspectives The researchers say that while their open-ended or "self-reporting" methodology to gauge student concerns about homework may have limitations – some might regard it as an opportunity for "typical adolescent complaining" – it was important to learn firsthand what the students believe. The paper was co-authored by Mollie Galloway from Lewis and Clark College and Jerusha Conner from Villanova University.
Clifton B. Parker is a writer at the Stanford News Service .
More Stories

⟵ Go to all Research Stories
Get the Educator
Subscribe to our monthly newsletter.
Stanford Graduate School of Education
482 Galvez Mall Stanford, CA 94305-3096 Tel: (650) 723-2109
- Contact Admissions
- GSE Leadership
- Site Feedback
- Web Accessibility
- Career Resources
- Faculty Open Positions
- Explore Courses
- Academic Calendar
- Office of the Registrar
- Cubberley Library
- StanfordWho
- StanfordYou
Improving lives through learning
- Stanford Home
- Maps & Directions
- Search Stanford
- Emergency Info
- Terms of Use
- Non-Discrimination
- Accessibility
© Stanford University , Stanford , California 94305 .

THE ALGONQUIN HARBINGER
- Excessive homework negatively impacts mental health, causes unnecessary stress

Caroline Lou
Opinion Editor Jula Utzschneider writes on the overwhelming chip on every student’s shoulder: homework.
Jula Utzschneider , Opinion Editor November 10, 2021
When the bell rings to end last period every day, I feel a sense of relief. However, this feeling soon wears off as I realize just how much work I have to do after the already-stressful school day ends.
While homework can be beneficial, more often than not, it is assigned excessively and unnecessarily. Teachers give a significant amount of homework, often due the next day. This causes students to spend far too much time doing such assignments and can be detrimental.
A 2013 study conducted at Stanford University found that students in top-performing school districts who spend too much time on homework experience more stress, physical health problems, a lack of balance in their lives and alienation from society. That study, published in The Journal of Experimental Education , suggested that any more than two hours of homework per night is counterproductive. However, students who participated in the study reported doing slightly more than three hours of homework every night.
And, yes, the amount of homework given to students depends on the course level they take. But, with increasingly competitive college acceptance rates (demanding more extracurriculars and college-level classes), many students feel forced to take these more challenging courses. This is a huge problem, especially as teachers give homework only thinking about their own class, not the five or six others students have.
Additionally, when it came to stress, more than 70% of students in the Stanford study said they were “often or always stressed over schoolwork,” with 56% listing homework as a primary stressor. More than 80% of students reported having at least one stress-related symptom (such as headaches, exhaustion, sleep deprivation, weight loss, stomach problems and more) in the past month, and 44% said they had experienced three or more symptoms.
Less than 1% of the students said homework was not a stressor, demonstrating that the vast majority feel overwhelmed and pressured by the amount of work they receive.
Not to mention, the time spent on these assignments could easily be spent doing something enjoyable. Many students feel forced or obligated to choose homework over practicing other talents or skills, which should never be the case. Teachers should be encouraging these extracurriculars, rather than making it impossible for students to partake in them.
In terms of what teachers can do, it’s quite simple, really. Homework is intended for students to either practice a subject further or to cover topics teachers couldn’t during the allotted class time. It should not be busywork that just wastes a student’s time.
Teachers should be giving students work that is absolutely necessary (not busy work), and eliminate it altogether where they can. It is extremely important that students not only get through high school but thrive and enjoy it too.
How much time do you spend doing homework on an average school night?
Sorry, there was an error loading this poll.
A donation of $40 or more includes a subscription to the 2023-24 print issues of The Harbinger. We will mail a copy of our fall, winter, spring and graduation issues to the recipient of your choice. Your donation supports the student journalists of Algonquin Regional High School and allows our extracurricular publication to purchase equipment and cover our annual website hosting costs.

Jula began writing for The Harbinger her freshman year after taking Journalism. While at first hesitant, she grew to love reporting and specifically opinion...

- Limitations are necessary for freedom of speech
- Mocking accents spreads unjust, offensive stereotypes
- The Great Debate: Should modern literature replace the classics in English class?
- The Director’s Eye: Heathers
- Students given too much homework, not enough time
What are you most excited for this summer?
- Going to the beach
- Pickleball 24/7
- Sleeping in
View Results
- Polls Archive

The official student news site of Algonquin Regional High School in Northborough, MA
- Corrections
Comments (3)
Cancel reply
Your email address will not be published. Required fields are marked *
m • May 4, 2023 at 12:41 pm
m • Jan 4, 2024 at 12:10 pm
sophia • Mar 8, 2023 at 1:57 pm
very true in fact i am writing a essay right now this is resurch
- The Great Debate
- Senior Issue
- Movies & TV
- Video Games
- Pro & College
- Cafe Takeaways
- Chicken Sandwich Chasers
- Club Detectors
- Hidden Gems
- The Racer Ru-view
- Print Issues
Homework and Mental health

In many ways, homework assignments seem like common sense. Spend more time repeating and practicing multiplication or studying Espanyol vocabulary, and you should master all the Spanish or math. Let’s now discuss Homework and Mental health and if it really impacts children’s health.
Table of Contents
1. Positive effects of Homework
Help students to master the coursework., help to cultivate proper problem-solving skills.
Students tend to develop better solving skills when given a chance to handle different questions independently, and the best way to induce this is by giving them some coursework to work at home .
Improve Retention and Understanding
2. negative effects of homework, induce boredom.

3. Contradictions about Homework and Mental health
4. acquisition of undesirable traits, 5. homework and mental health statistics.
The findings on homework relation to mental health were so troubling since the report showed that too many homework tasks are associated with high levels of stress, physical health condition, and lack of balance in students’ lives.
Fifty-seven percent of the children in the research cited that homework as primary anxiety and stressor in their schooling life (Langberg, J. M., Dvorsky, M. R., Molitor, S. J., Bourchtein, E., Eddy, L. D., Smith, Z. R., … & Eadeh, H. M.).
When it comes down to stress and health, it is clear that too much homework for a student at both ends of the learning spectrum can be of significant damage, which brings the question of how much homework is too much for an average or typical student?
6. What experts have to say about homework and mental health
While many researchers have tried to give their view on how much is too much assignment, the National Education Association and the PTA recommend that students and learners spend 20 minutes per grade per night.

Final summary on Homework and Mental health
With all facts at hand, we can conclude that homework plays a huge role in stimulating our kid’s ability to solve problems and also to seek independence in life, but we cannot forget the negative side they have to hold and keep up with. Stress is one of the critical contributors coming from pressuring students to find answers, and the best way to solve that is to always assign students assignments in fields they like.
Share this:
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
August 12, 2024
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
reputable news agency
How excessive heat can affect your mental health
by Robin Foster

As Americans sweat through another scorching summer, one expert warns that while extreme heat can cause physical harm, it can also wreak havoc with your mental health.
Sizzling temperatures can make anyone irritable, but it can be far worse for some, especially those with mental health conditions, said Dr. Asim Shah, executive vice chair in the Menninger Department of Psychiatry and Behavioral Sciences at Baylor College of Medicine in Houston.
Excessive heat can trigger feelings of anger, irritability, aggression, discomfort, stress and fatigue because of its impact on serotonin, the neurotransmitter that regulates your sleep, mood and behaviors, Shah noted.
The most vulnerable groups include people with preexisting mental health conditions and people who abuse alcohol or other drugs.
"All mental illnesses increase with heat because it results in more fatigue, irritability and anxiety, and it can exacerbate depressive episodes," Shah explained in a Baylor news release.
What are the signs of impending trouble? They tend to start with irritability, decreased motivation, aggressive behavior and sometimes mental fogging. In worse cases, confusion and disorientation occur, Shah noted.
While avoiding the heat may not be possible, Shah recommends hydrating and keeping your head covered when going outside. If it gets too hot, pour some water on your head to cool down and try doing things in the shade. If you normally go for walks outside, try walking in the mall or a large space with air conditioning.
If you take medications, consult with your provider because some medications for mental health, such as lithium for bipolar patients, don't pair well with heat. Lithium goes through the kidney, so sweating can have an impact on the levels of the medication in your body, Shah explained.
"If you are out in the heat and using lithium, levels may fluctuate. In that scenario, we have to be very careful and either adjust the dosage of lithium or avoid heat," he noted.
Droughts and extreme changes in temperature can also increase levels of pollutants and allergens as air quality worsens. That can exacerbate mental health issues like depression, anxiety or PTSD. Some studies show that exposure to any natural climate disaster can raise the risk of depression by more than 30%, anxiety by 70% and both by over 87%, Shah said.
Kids are not immune to the effects of intense heat, either.
"Children are a vulnerable population due to their physical and cognitive immaturity. They are exposed to more pollutants and allergens as they spend more time outdoors," Shah noted.
If you feel affected by severe heat, call your doctor or mental health specialist.
Copyright © 2024 HealthDay . All rights reserved.
Explore further
Feedback to editors

Australia offers lessons for increasing American life expectancy
8 hours ago

Childhood maltreatment is associated with greater cognitive difficulties than previously thought

Lack of purpose and personal growth in older age may precede mild cognitive impairment

Two new studies show how immunotherapies collaborate to boost T cell responses in melanoma
10 hours ago

Could targeting metabolism treat blood clots in antiphospholipid syndrome?

New research explores the urea cycle's strong connection to fatty liver disease

Clinical trial shows JAK inhibitor improves multiple autoimmune conditions in patients with Down syndrome
11 hours ago

Stroke prevention trials should include patients with disabilities, study says
12 hours ago

Study finds preterm-born children fit into three profiles, with different results in cognition and behavior tests

First genome-wide comparison of vapers and smokers finds similar DNA changes linked to disease risk
13 hours ago
Related Stories

Excessive heat and its impact on mental health
Jul 24, 2023

Spotting the silent symptoms of stress
May 6, 2024

One year later: The impact of Hurricane Harvey on mental health
Aug 16, 2018

Understanding effects of heat on mental health
Jul 14, 2023
Dealing with the psychological aftermath of Hurricane Harvey
Sep 1, 2017

Take a deep breath: how to cope with panic attacks
Apr 24, 2019
Recommended for you

Hand washing is important—but is your handbasin clean?
14 hours ago

Emergency cash payments found to have positive impact on vulnerable young Australians
16 hours ago
Let us know if there is a problem with our content
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
- Open access
- Published: 06 August 2024
Mindfulness, teacher mental health, and well-being in early education: a correlational study
- Carolina Corthorn 1 ,
- Víctor Pedrero 2 ,
- Natalia Torres 1 ,
- Katiuska Reynaldos-Grandón 2 &
- Paola Paredes 3
BMC Psychology volume 12 , Article number: 428 ( 2024 ) Cite this article
260 Accesses
Metrics details
This study analyzed the relationship between mindfulness and variables considered relevant for teacher–student interactions: teacher burnout, general stress, anxiety, depression, and quality of life. We hypothesized that mindfulness would relate negatively with mental health variables and positively with quality of life. We also explored which specific aspects of mindfulness would predict burnout, depression, anxiety, stress, and quality of life. Given the results of regression analyses, mediation models were performed to explore the mechanisms through which different facets of mindfulness affect quality of life. As predicted, the correlation analysis showed that mindfulness and its dimensions were positively associated with the quality of life of the teachers and burnout dimension of personal fulfillment and negatively associated with anxiety, depression, and stress (considering FFMQ total score and most of its dimensions). Consistently, regression analysis showed that the overall level of mindfulness, after controlling for the grade level at which the teacher works, showed significant associations with the level of personal fulfillment, depression, anxiety, stress, and quality of life. The results of the mediation analyses showed that the ability not to judge ourselves was associated with fewer symptoms of depression and stress and, through these pathways, positively affected quality of life. On the other hand, the ability not to react favored quality of life by reducing anxiety and stress. Finally, acting with awareness was the only facet of mindfulness that favored quality of life, affecting one of the dimensions of burnout.
Peer Review reports
The measurement of quality in early childhood education considers factors related to structure and process. Structure-related factors refer to minimum conditions such as supplies, infrastructure, and the adult/child ratio. Process-related factors refer to teacher-child interactions where learning takes place and for which teachers’ sensitivity and socioemotional skills are essential [ 1 , 2 , 3 , 4 , 5 ]. Teachers who are aware of and receptive to children’s signals regarding both their emotional and cognitive needs can provide better quality interactions favoring the development of the children under their care. One factor that can significantly affect process-related factors is the teacher’s mental health and well-being. Evidence shows that teaching is a highly stressful occupation [ 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 ]. This risk factor is even more concerning considering the actual post-pandemic scenario. As a general context, COVID-19 has generated a mental health crisis internationally, with an increase in both acute and chronic stress levels. It is estimated that the increase in anxiety and depression disorders was more than 25% during the first year of the pandemic [ 15 ]. Regarding the context where this research was conducted, during pandemic and post-pandemic period 25% of Chileans presented symptoms of anxiety [ 16 ] and 67% of work-related illnesses identified during 2022 were mental health diagnoses [ 17 ] Also, pandemic and post pandemic context has had an impact in teacher’s labor conditions. During the pandemic 63% of Chilean teachers considered their workload increased and 85% reported feeling “stressed or very stressed” [ 18 ]. 49% of teachers in Chile perceive that class climate became worse in 2022, compared to 2021. They report an average of 9 extra nonpaid worked hours per week [ 19 ]. Literature is clear regarding the relation among excessive workload and teacher’s well-being and mental health [ 20 , 21 ]. In Chile, this aspect might be of particular concern since it appears to be affecting teacher retention in the school system. It has been found that 20,2% of new teachers desert their job in their 5th year of work [ 22 ]. Studies project an important deficit of teachers in Chilean schools by the year 2030 [ 23 ].
Work stress not only affects the physical and mental health of the teacher, but symptoms of burnout, such as irritability, discouragement and hyperreactivity to stress, represent serious interference in the teacher-student relationship and therefore affect the effectiveness of the teaching-learning process [ 24 ]. An unmotivated and irritated teacher who is working with great emotional distance, trying to mitigate the negative effects she perceives her work is having on her emotional well-being, can generate a very negative impact on interactions in the classroom [ 25 ]. Therefore, the relevance of promoting teachers’ mental health and well-being is warranted. Schonert-Reichl [ 5 ] proposes that this should be included as part of teacher preparation and professional development, which should not only include contents about children’s social and emotional learning and development, but also give teachers tools and strategies to develop their own socio-emotional well-being. Teacher’s mental health should be considered a priority not only because of its impact in children, but also since this is a fundamental human right as defined by the World Health Organization (WHO) [ 26 ]. Therefore, we must seek to ensure healthy work environments for teachers, which includes taking into account not only teachers’ socio-emotional personal development but also generating adequate work conditions and an educational structure that value the work of teachers.
WHO [ 26 ] defines mental health as an aspect that is an integral part of our health and general well-being. It points out that by having mental health, people have a better ability to relate, function, face difficulties and thrive. In turn, it maintains that mental health exists on a continuum, with experiences ranging from an optimal state of well-being to debilitating states of great suffering and emotional pain. Likewise, WHO states that health is not defined merely by the absence of disease, but rather proposes a holistic promotion approach towards health and its care. In this context, it raises the concept of quality of life and emphasizes the importance of measuring and evaluating it to have a proactive and preventive perspective. It defines quality of life as the perception that an individual has about his position in life in the context of his culture and value system in which he lives and how this relates to his goals, expectations, standards and concerns [ 27 ].
Mindfulness, defined as an awareness that arises through “paying attention in a particular way, on purpose, in the present moment, non-judgmentally” [ 28 ] has been widely used as an evidence-based practice for approaching the improvement of mental health and well-being. Empirical studies show that the benefits of mindfulness are abundant, including reducing stress, increasing positive emotions, and improving quality of life. Meta-analytical studies report significant results in reducing depression and anxiety, with effect sizes ranging from medium to large [ 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 ]. At the interpersonal level, improvements are observed in the quality of interpersonal relationships and intimacy [ 37 , 38 ], identification and communication of emotions, anger management, and empathy [ 39 ]. Finally, at the cerebral level, effects of mindfulness-based interventions have been found in areas of the brain associated with the experience of positive emotions [ 40 ] and with empathy and theory of mind [ 41 ]. Structural brain changes have been found in areas associated with learning and memory processes, emotional regulation, self-referential processing, and perspective taking after participating in a mindfulness-based intervention (MBSR) [ 42 ]. In terms of neuroendocrine responses, Brown, Weinstein, and Creswell [ 43 ] found that individuals who had higher levels of mindfulness also had lower levels of cortisol and perceived stress.
Considering the abundant evidence regarding the effects of mindfulness on stress reduction, well-being, emotional regulation, health, and prosocial dispositions [ 29 , 30 , 31 , 32 , 33 ] there has been an increased interest in developing adaptations of mindfulness programs for the school context. For example, helping teachers cultivate mental habits would help them be better prepared for job-related demands and stressors. It has been proposed that training teachers in mindfulness would help to strengthen their resilience and prevent burnout [ 44 , 45 , 46 ]. Additionally, they can transmit this tool to their students either by modeling attitudes and behaviors that embody mindfulness and/or through direct instruction of mindfulness practices directed to the children. Evidence shows that mindfulness helps to promote the development of children’s executive functions and the self-regulation of emotions and impulses [ 44 ]. The ability to regulate attention and emotions provides a basis for school readiness, as it enhances dispositions that are conducive to learning and that promote positive interpersonal relationships [ 47 ]. Longitudinal studies show that self-regulation in childhood is a key predictor of health, financial stability, and educational achievement in adulthood [ 48 ]. Therefore, implementing mindfulness in educational contexts would be positive for both children and teachers, together with the educational community.
Most studies regarding mindfulness in education assess the results of mindfulness-based interventions directed either to teachers or students and find significant effects on several measures. For instance, a meta-analysis that reviewed 24 studies evaluating mindfulness in the school context found effect sizes (Hedge’s g) of 0.80 for cognitive performance (mainly tests of attention and concentration), 0.39 for stress reduction, and 0.36 for measures of resilience [ 49 ]. A systematic review of 16 studies of mindfulness interventions for in-service teachers found positive effects (Cohen’s d) on teacher wellbeing, including reduction of perceived stress and burnout (size effect from 0.24 to 0.90), physiological symptoms of stress (cortisol levels, d = 0.70), depression (effect size from 0.61 to -1.06), anxiety (effect size from 0.71 to 0.89) and overall psychological distress (effect size from 0.53 to 1.74). Additionally, they found positive effects on classroom organization (d = 0.28), teacher’s sense of efficacy (d from 0.52 to 0.66) and use of positive affect words in the classroom (d = 0.57). [ 50 ] In a more recent systematic review, Hidajat et al. [ 51 ] evaluated the efficacy of mindfulness-based interventions for teachers’ stress and burnout outcomes. They found that 77%, 20 out of 26 studies, reported a significant reduction in stress and 89%, 16 out of 18 studies, a significant reduction in burnout.
At the preschool level, studies have also found significant effects of mindfulness-based interventions on measures of executive functions [ 52 , 53 , 54 ], self-regulation [ 54 , 55 , 56 ], prosocial behavior [ 44 , 57 , 58 , 59 ], resilience [ 59 ] and hyperactivity [ 44 , 58 , 60 ]. Jackman et al. [ 61 ] also reported an increase in body and emotional awareness, self-calming skills, and empathy. Some studies also report evidence regarding reduced perceived stress in early childhood teachers as an effect of mindfulness-based interventions [ 62 , 63 , 64 ].
Studies at the preschool level have also shown that children from disadvantaged sectors benefit more from mindfulness interventions in social-emotional and behavioral areas. These findings could be especially beneficial in countries with higher social inequality, such as Chile. In this sense, Poehlmann-Tynan et al. [ 55 ] show that a mindfulness intervention significantly increased attentional focus and self-regulation among young children from economically disadvantaged families. Another study regarding mindfulness and executive functions points out that children from lower socioeconomic backgrounds show lower levels of executive functions and higher levels of stress and stress hormones. Since stress interferes with the use and development of those skills, mindfulness intervention could be significantly beneficial for them [ 53 ].
These kinds of studies provide substantial evidence regarding the effects of mindfulness-based programs in the educational setting. Nevertheless, interventions are usually complex and include several factors intrinsic to their characteristics, making it difficult to be certain about what specific aspects generated the results. Was it mindfulness per se? Was it being listened to in the context of a group practice? Was it sharing experiences with others? Was it having a supportive and attentive instructor? Considering the complexity of intervention scenarios, it is also interesting to approach the study of mindfulness in education by analyzing the relation among mindfulness as a ‘‘trait’’ and variables related to teachers’ mental health and well-being, which, as previously mentioned, is a fundamental variable for assuring good teacher-student interactions and is therefore essential for the quality of the learning process. Identifying relevant aspects associated with being more mindful provides further evidence regarding the importance of mindfulness, regardless of meditation practice. Studies focused on general population samples have found that people who are naturally more mindful report feeling less stressed, anxious, or depressed and happier, inspired, grateful, self-compassionate, and satisfied with life [ 37 , 65 , 66 , 67 , 68 , 69 ]. People with a higher level of mindfulness have also been found to have greater awareness of their emotional states, greater understanding and acceptance of them, and better emotional self-regulation [ 31 , 67 , 70 ]. Regarding teachers, there are also some studies that assess the relation among mindfulness and other variables without intervention. For instance, Becker, Gallagher and Whitaker [ 71 ] analyzed the relation between the dispositional mindfulness of early childhood educators and the quality of teacher-child interactions, finding a positive relation among them. In another study, Anama-Green [ 72 ] analyzed the relationship among the self-reported levels of burnout and secondary traumatic stress of teachers and their reported levels of interpersonal and intrapersonal mindfulness. Those who reported high intrapersonal mindfulness scores were up to 11 times more likely to report “low” burnout than those who reported low intrapersonal mindfulness scores. Studies that measure mindfulness as a “trait” can be a very valuable source of scientific data, but it is important to keep in mind that mindfulness is a skill that can be developed through practice, as mentioned in previous paragraphs.
The purpose of the present study was to analyze the relationship between mindfulness and variables considered relevant for teacher–student interactions: teacher burnout, general stress, anxiety, depression, and quality of life. We hypothesized that mindfulness would relate negatively with mental health-related variables – teacher burnout, stress, anxiety, and depression – and positively with quality of life as perceived by the teachers in self-report questionnaires. We also explored which aspects of mindfulness would predict lower levels of burnout, depression, anxiety, and stress. Finally, we also explored which aspects of mindfulness are specifically related to quality of life.
Materials and methods
Participants.
The participants of this study were 42 preschool teachers and teacher assistants who work at public schools and preschool centers administered by a local municipality in the city of Santiago, Chile (Municipalidad de La Reina). The average age of the teachers ( n = 27) and teacher assistants ( n = 15) was 40 years old (SD = 14); most of them were women ( n = 41), married (38.1%), worked in the school context for an average of 14 years (45.2%), and had an average of 26 children in their classes (SD = 8) (See Table 1 for detailed sample description).
The participants were invited to the study during an online meeting where the study was fully explained, together with the main principles of mindfulness and its benefits, and they were also informed that their participation would be voluntary and confidential. First, we contacted by mail the director of the board of education of La Reina, Chile, who facilitated the meeting in which the early childhood teachers and the school principals learned about the proposal. The letter of consent and the questionnaires were sent to the participants by email using a Google Form. To ensure the return of both forms, participants received a weekly reminder by mail; earlier letters were generic, and later letters were addressed to specific individuals.
Sociodemographic questionnaire
The participants completed a questionnaire regarding contact and sociodemographic information, including the following aspects: date of birth, gender, marital status, occupation, type of contract, number of years working as a preschool teacher or assistant, type of center they worked in (school v/s preschool center), number of hours worked daily, number of children in their classrooms, and level they taught.
Five-facet mindfulness questionnaire
The FFMQ is a 39-item measure that assesses five mindfulness domains [ 65 ] . Scores range from 1 = Never or rarely true to 5 = Very often or always true , where higher scores reflect more mindfulness in five aspects. Subscale observing (α = 0.78) measures the tendency to notice or attend to internal and external experiences, such as emotions, cognitions, sights, and smells. Describing (α = 0.90) measures the tendency to verbally describe and label these experiences. Acting with awareness (α = 0.87) refers to bringing full awareness to current activity or experiences. Nonjudging (α = 0.82) refers to a nonevaluative stance toward inner experiences. Nonreactivity (α = 0.79) measures the tendency to allow thoughts and feelings to come and go without getting carried away by them. The construct validity of the FFMQ has been extensively assessed in meditating and nonmeditating samples [ 65 , 70 ]. In Chile, good reliability has also been found; α = 0.91 for the general scale, and scores range from 0.75 to 0.88 in Cronbach’s alpha for the five subscales [ 73 ].
The Depression Anxiety Stress Scales 21 (DASS-21) is a short form of Lovibond and Lovibond’s [ 74 ] 42-item self-report measure of depression, anxiety, and stress (DASS). The DASS consists of three 14-item self-report scales. A 4-point severity scale measures the extent to which each state has been experienced over the past week. The DASS-21 consists of three 7-item self-report scales taken from the full version of the DASS. The depression scale (α = 0.86) assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia, and inertia. The anxiety scale (α = 0.8) assesses autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious affect. The stress scale (α = 0.82) is sensitive to levels of chronic, nonspecific arousal. It assesses difficulty relaxing, nervous arousal, and being easily upset/agitated, irritable/overreactive, and impatient. Scores can be grouped into ranges according to severity: normal , mild , moderate , severe , and extremely severe . These labels are used to characterize the full range of scores in the population. For example, “mild” means that the person is above the population mean but still well below the typical severity of people seeking help (it does not mean a mild level of a “disorder”). The DASS-21 was translated and adapted in Chile, and psychometric studies support its use in the Chilean population [ 75 , 76 ].
Quality of life questionnaire (WHOQOL-BREF)
This is a questionnaire developed by the World Health Organization that provides a self-reported profile of quality of life. It was designed to be used in both the general and clinical populations. There are two versions, the WHOQOL-100 and the WHOQOL-BREF, both with validation studies in Spanish. The version used in this study is the brief version, that is, the WHOQOL-BREF (α = 0.88), which provides a quick way to score the profiles it explores, and consists of a self-administered questionnaire of 26 questions, with 5 response alternatives in Likert scale (1 to 5) and generates a profile of 4 dimensions that are scored independently, namely, physical health, psychological health, social relationships and environment, as well as a global score on perception of quality of life and general health. The higher the score is, the better the quality-of-life profile of the person evaluated is.
Maslach burnout inventory-educators survey (MBI-ES)
The Maslach Burnout Inventory (MBI) developed by Maslach and Jackson [ 77 ] is validated by extensive research that has been conducted in the more than 35 years since its initial publication. The MBI-ES is a 22-item self-report version of the original MBI for use with educators, including teachers, administrators, other staff members, and volunteers working in any educational setting. The MBI-ES addresses three scales: emotional exhaustion (α = 0.79) measures feelings of being emotionally overextended and exhausted by one’s work, depersonalization (α = 0.4) measures an unfeeling and impersonal response toward recipients of one’s instruction, and personal accomplishment (α = 0.76) measures feelings of competence and successful achievement in one’s work.
Data analyses
The statistical analysis was performed using IBM SPSS Statistics for Macintosh, Version 28.0. Armonk, NY: IBM Corp. Descriptive analyses of FFMQ (mindfulness), Maslach (teacher burnout), DASS-21 (depression, anxiety, and stress) and WHOQOL (quality of life) were performed. Next, we obtained Spearman correlation analysis among the instruments and sociodemographic variables (age, years working as a preschool teacher, number of children in classroom, grade they teach in). Additionally, multiple regression analyses were performed to evaluate the relationship between FFMQ subscales and the different variables in this study: teacher burnout, stress, anxiety, depression, and quality of life. The regression models were adjusted for those variables that showed a significant correlation ( p < .05) with at least one of the dependent variables. Each model added the FFMQ subdimensions in a single step. Finally, we explored whether the relationship between the level of mindfulness and the participant’s quality of life was mediated by the level of burnout, anxiety, depression, or stress. The mediation analysis considered the global score of the FFMQ and its dimensions that showed significant associations with the Maslach inventory or DASS in the regression analysis and a significant relationship between the Maslach inventory or DASS and quality of life in the correlation analysis. According to recent recommendations, the relationship between FFMQ and quality of life would be nonnecessary to perform a mediation analysis [ 78 , 79 ]. Due to the small sample size and the distributions of the variables, 95% bootstrap confidence intervals were estimated for regression analysis and mediation models.
Descriptive analyses
The preschool teachers and teacher assistants who participated in the present study obtained an average score of 133 (SD = 24) in mindfulness (total FFMQ score) and 90 (SD = 12.5) in quality of life (total WHOQOL-BREF score). DASS-21 average scores were on average within normal ranges (below the population mean): depression 2.5 (SD = 3.1), anxiety 3.5 (SD = 3.6), and stress 3.5 (SD = 3.2). Regarding sample distribution, 80.9% of participants were within normal ranges for depression, 59.5% for anxiety, and 83.3% for stress. Participants in the mild and moderate categories were 14.3% for depression, 28.6% for anxiety, and 14.3% for stress. Severe score ranges were obtained by 4.8% of participants for depression and 7.1% for anxiety. No severe scores were obtained for stress. Extremely severe scores were obtained only for anxiety by 7.1% of the participants. It is important to note that 14.2% of the preschool teachers and teachers’ assistants presented severe to extremely severe levels of anxiety according to the DASS-21. Regarding teacher burnout scores, in Maslach’s subscales, the participants obtained 21 (SD = 6.6) for emotional exhaustion, 6 (SD = 2.4) for depersonalization, and 40 (SD = 6.5) for personal accomplishment. MBI scores are considered low between 1 and 33 points, medium between 34 and 66 points, and high between 67 and 99. Therefore, participants were, on average, at medium levels of emotional exhaustion, low levels of depersonalization and high levels of personal accomplishment. Regarding sample distribution, 19% of the participants presented high levels of emotional exhaustion and 10% of depersonalization. 7% of the sample presented low levels of personal accomplishment.
Correlation analyses
The correlation analysis showed that both the total score of the FFMQ and its dimensions were positively and significantly associated with the level of quality of life of the teachers (Table 2 ). The magnitude of these correlations ranged from r s = 0.37, p = .016 for the relationship between awareness and quality of life and r s = 0.7 for the relationship between the global level of mindfulness and quality of life. Regarding the relationship between mindfulness, anxiety, depression, and stress, we observed negative and significant associations in almost all cases, both when considering the total score of the FFMQ and its dimensions. Two exceptions were the relationship between observation and stress (r s = –0.21, p = .174) and that between depression and awareness (r s = –0.17, p = .271). We observed no relationship between the dimensions of the FFMQ and two of the dimensions of burnout: emotional exhaustion and depersonalization. However, there was a positive and significant relationship between the burnout dimension of personal fulfillment and the following FFMQ dimensions: describe (r s = 0.4, p = .008), awareness (r s = 0.44, p = .003) and nonjudgment (r s = 0.4, p = .009). The overall level of mindfulness was also significantly associated with the level of personal fulfillment (r s = 0.59, p < .001). Finally, the level of quality of life was negatively correlated with anxiety (r s = − 0.55, p < .01), depression (r s = –0.71 p < .001), stress (r s = –0.68, p < .001) and emotional exhaustion (r s =–0.37 p = .015). The level of personal fulfillment was positively associated with quality of life (r s = 0.49, p = .001), and no association was observed between quality of life and depersonalization (r s = − 0.12, p = .45). Regarding the sociodemographic variables, only significant associations were observed between the level at which the teachers worked, emotional exhaustion (r s =0.4 p = .009) and anxiety (r s = − 0.32, p = .037). This variable was included as a control variable in the regression models.
Regression analyses
The overall level of mindfulness, after controlling for the grade level at which the teacher works, showed significant associations with the level of personal fulfillment (B = 0.2; 95% CI [0.11; 0.3]), depression (B = -0.1; 95% CI [-0.15; -0.05]), anxiety (B = -0.13; 95% CI [–0.19, -0.08]), stress (B = -0.12; 95% CI [–0.17; − 0.07]) and quality of life (B = 0.52; 95% CI [0.39; 0.62]). When analyzing the association between the facets of mindfulness and the level of anxiety, depression, and stress, it was observed that having a nonjudgmental attitude toward oneself was significantly related to the degree of depression (B = − 0.22; 95% CI [–0.39; − 0.04)] and stress (B = − 0.22, 95% CI [–0.37; − 0.03]). Nonreact showed a significant negative effect on stress (B=–0.28; 95% CI [–0.53; − 0.04]) and anxiety (B= − 0.35; 95% CI [–0.63; − 0.05)]). Only the ability not to judge oneself positively affected quality of life after controlling for the other facets of mindfulness (B = 0.95; 95% CI [0.37;1.62]). Consistent with the findings in the correlation analysis, we observed no significant association between the dimensions of the FFMQ and emotional exhaustion or depersonalization (Table 3 ). Regarding personal fulfillment, only awareness was significantly associated with this domain (B = 0.4; 95% CI [0.01, 1.04]).
Mediation models
Given the results obtained in regression analysis, different mediation models were performed (Fig. 1 ). First, we analyzed the mediating role of personal fulfillment, anxiety, depression, and stress in the relationship between the global level of mindfulness and quality of life. In these models, we observed a significant mediating role of depressive symptoms (indirect effect = 0.17; 95% CI [0.55, 0.33]) and stress level (indirect effect = 0.18; 95% CI [0.09; 0.3]), while anxiety level (indirect effect = 0.07; 95% CI [–0.5; 0.19]) and degree of personal fulfillment ( indirect effect = 0.03; 95% CI[–0.05;0.15]) did not have a mediating role in this relationship. Then, we explored the mediating role of the level of depression and stress in the relationship between a person’s ability not to judge themselves and their quality of life. The results of this analysis show that both depression (indirect effect = 0.5; 1 95% CI [0.13, 0.87]) and stress (indirect effect = 0.57; 95% CI [0.23; 0.98]) significantly mediate this relationship. Additionally, we explored the mediating role of anxiety and stress in the relationship between nonreact and quality of life, although in this case, no association was observed between nonreact and quality of life in the regression analysis; however, in the correlation analysis, we can observe a significant relationship. According to O’Rourke (2018), there are several situations where the total effect is not significant, and the mediation effect is significant. One of these cases is when both effects are equivalent (complete mediation); in this scenario, the power to detect the mediation effect would be higher than the power to detect the total effect, especially with large effects in small samples. In this research, we have a small sample and a relatively large effect in the correlation analysis but no relationship between nonreact and quality of life in the regression analysis. The mediation analysis showed that both anxiety (indirect effect = 0.69; 95% CI [0.25;1.22]) and stress (indirect effect = 0.67; 95% CI [0.24; 1.24]) totally mediated this relationship, compatible with O’Rourke’s assumption. Finally, we analyzed whether personal fulfillment mediated the relationship between act with awareness and quality of life. In the latter case, we observed that personal fulfillment completely mediated this relationship ( indirect effect = 0.37; 95% CI [0.05, 0.74]). Together, these results show that there are variations in the mechanisms through which the different facets of mindfulness affect quality of life. The ability not to judge ourselves is associated with fewer depressive symptoms and stress, and it positively affects quality of life through these pathways. On the other hand, the ability not to react favored quality of life by reducing anxiety and stress. Finally, acting with awareness is the only facet of mindfulness that favors quality of life by affecting one of the dimensions of burnout.

Mediation analysis
The present study is coherent with previous evidence regarding a positive relationship between mindfulness and quality of life and a negative relationship between mindfulness and variables related to teachers’ mental health (depression, anxiety, and stress). The results contribute to this line of research by analyzing in a more specific way how these relations occur, that is, whether mindfulness and quality of life are directly related or if it is a mediated relation through reducing the effects of mental health-related variables. Furthermore, exploring what specific dimensions of mindfulness can be involved in this process.
As mentioned, a positive significant relation was found between mindfulness and the burnout dimension of personal fulfillment but not with the other dimensions of burnout (emotional exhaustion and depersonalization). The findings of the present study were consistent with previous research that found the FFMQ’s nonjudging dimension to be a main predictor of mental health and quality of life. For instance, Cash and Whittingham [ 80 ] also performed a multiple regression analysis to determine which aspects of mindfulness as measured in the FFMQ would predict depression, anxiety, and stress, as measured by the DASS-21. They found that the main predictor was nonjudging. Additionally, Baer et al.’s [ 65 ] findings showed that nonjudging had the highest correlations with psychological symptoms, neuroticism, thought suppression, difficulty regulating emotion, and experiential avoidance compared to all other mindfulness facets. In another study focused on the relations among mindfulness and parenting variables, Corthorn and Milicic [ 81 ] found that nonjudgmental acceptance of self (FFMQ) and nonjudgmental acceptance of self as a mother (IM-P) were the main predictors of mothers’ levels of mental health as measured by the DASS-21, and nonjudgmental acceptance of self as a mother was also a main predictor of lower levels of parental stress. In a more recent study, Ortet et al. [ 82 ] found that the nonjudging facet of the FFMQ is a significant predictor of subjective well-being when personality is accounted for, suggesting that mindfulness training that intends to improve subjective well-being should focus on the nonjudging dimension.
As mentioned before, it was found that the ability not to react favored quality of life by reducing anxiety and stress. Some studies have found a relationship between nonreact and anxiety symptoms. For example, Diehl et al. [ 83 ] found that increased reactivity to experiences was more closely associated with generalized anxiety symptoms, while acting with awareness was associated with depressive symptoms.
Additionally, in line with the findings, the mediational models of the present study found, as presented in the results section, that mindfulness and quality of life would be mediated by how the former affects symptoms of stress and depression. Furthermore, particularly relevant in the mediation, the FFMQ dimensions of nonjudging and nonreacting provided additional evidence related to the probable importance of nonjudging regarding its effects on mental health variables and how this relation affects the quality of life of teachers.
One of the main methodological limitations of this study is the small sample size. This can limit the generalization of the results, interfere with the estimates due to the low power to detect some relationships and possible problems in estimating confidence intervals. Despite this, previous studies in mediation models have suggested that even with samples between 34 and 50 participants [ 84 ], it is possible to maintain acceptable type I error rates using bootstrap methods such as those used in this study [ 85 ]. In the future, studies with a larger sample size would be necessary to confirm the results obtained. Another limitation of this study is the low reliability of the depersonalization subscale of Maslach’s inventory in the sample, therefore the level of depersonalization should be interpreted with caution. Also, this finding could contribute to explain the absence of significant results when this variable is used in different statistical analysis. To assess the role of this variable a latent variable approach could be appropriated but the small sample size did not permit this.
It would be interesting in future studies to address possible differences in samples from other municipalities and regions within Chile and also comparison with other Latin American countries, to evaluate if and how contextual factors affect the results. For example, studies in rural areas where the risk and protective factors that affect mental health are different from those in urban areas, where the present study was conducted. [ 86 , 87 ].
Considering the positive results in the present study regarding mindfulness and its relationship with mental health and quality of life, we also suggest future studies could evaluate the effects of mindfulness-based interventions focused on preschool teachers in similar contexts.
Data availability
The data that support the findings of this study are available from the authors upon reasonable request.
Doherty G, Forer B, Lero D, Goelman H, La Grange A. Predictors of quality in Family Childcare. Early Child Res Q. 2006;21(3):296–312.
Article Google Scholar
Hamre B. Teachers’ daily interactions with children: an essential ingredient in effective early Childhood Programs. Child Dev Perspect. 2014;8(4):223–30.
Jennings PA, Greenberg M. The Prosocial Classroom: teacher social and emotional competence in relation to child and classroom outcomes. Rev Educ Res. 2009;79:491–525.
Jennings PA. Early childhood teachers’ Well-being, Mindfulness, and Self-Compassion in Relation to Classroom Quality and attitudes towards challenging students. Mindfulness. 2014;6(4):732–43.
Schonert-Reichl K. Social and emotional learning and teachers. Future Child. 2017;27(1):137–55.
Barford SW, Whelton WJ. Understantding burnout in child and Youth Care workers. Child Youth Care Forum. 2010;39:271–87.
Clipa O, Boghean A. Stress Factors and Solutions for the Phenomenon of Burnout of Preschool teachers. Procedia- Social Behav Sci. 2015;180:907–15.
Farewell CV, Quinlan J, Melnick E, Powers J, Puma J. Job demands and resources experienced by the early Childhood Education workforce serving high-need populations. Early Childhood Educ J. 2021;50(2):197–206.
Kahn WA. Caring for the caregivers: patterns of organizational caregiving. Adm Sci Q. 1993;38(4):539–64.
Sautelle E, Bowles T, Hattie J, Arifin DN. Personality, resilience, self-regulation and cognitive ability relevant to teacher selection. Australian J Teacher Educ. 2015; 40(4).
Travers CJ, Cooper CL. Mental Health, Job satisfaction and occupational stress among UK teachers. Work Stress. 1993;7(3):203–19.
Young KM, Cooper CL. Change in stress outcomes following an industrial dispute in the ambulance service: a longitudinal study. Health Serv Manage Rev. 1999;12:51–62.
Li S, Li Y, Lv H, Jiang R, Zhao P, Zheng X et al. The prevalence and correlates of burnout among Chinese preschool teachers. BMC Public Health. 2020; 20(160).
Wagner SL, Forer B, Cepeda IL, Goelman H, Maggi S, D’Angiulli A, et al. Perceived stress and Canadian early childcare educators. Child Youth Care Forum. 2013;42:53–70.
World Health Organization. Mental Health and COVID-19: early evidence of the pandemic’s impact. Scientific brief. World Health Organization; 2022.
Bravo D, Errázuriz A, Campos D, Calfucoy P. Térmometro de la salud mental en Chile ACHS-UC: Octava Ronda. [Online].; 2024 [cited 2024 Junio 10. http://www.achs.cl/docs/librariesprovider2/2024/achs-221357/termometro-de-la-salud-mental-en-chile-achs-uc-octava-ronda.pdf
Superintendencia de Seguridad Social (SUSESO). Informe Anual 2022 de Seguridad Y Salud en El Trabajo. Informe Anual. Santiago, Chile: Superintendencia de Seguridad Social, Unidad de Estudios y Estadísticas; 2023.
Google Scholar
Elige Educar. Situación de docentes y educadores en contexto de pandemia. Necesidades y proyecciones para la labor docente en el marco del escenario sanitario vigente. Informe de Resultados. Santiago de Chile:; 2021.
Elige Educar. Encuesta Nacional: Voces Docentes VI, Sexta versión. Reporte De Resultados. Santiago de Chile: Elige Educar; 2023.
Jin P, Yeung A, Tang TO, Low R. Identifying teachers at risk in Hong Kong: psychosomatic symptoms and sources of stress. J Psychosom Res 2008 Oct; 65(4): p. 357–62.
Timperley H, Robinson V. Workload and the Professional Culture of teachers. Volume 28. Educational Management Administration & Leadership; 2000 January. 1.
Elige Educar. Resumen Ejecutivo: Retención, rotación, salidas de aula y reincorporación docente. Resumen Ejecutivo. Santiago de Chile: Elige Educar; 2022.
Elige Educar. Análisis y proyección de la dotación docente en Chile. Santiago de Chile: Elige Educar; 2021.
Mason O. Le syndrome d’epuisement professional: Burnout. Thérapie Familiale Geneve. 1990;11(4):335–70.
Arón A, Milicic N. Desgaste Profesional De Los profesores y clima social escolar. Revista Latinoam De Psicología. 2000;32(3):447–66.
World Health Organization (WHO). World mental health report: transforming mental health for all. Geneva: World Health Organization; 2022.
World Health Organization. The World Health Organization Quality of LIfe (WHOQOL). World Health Organization, WHOQOL Group;; 2012.
Kabat-Zinn J. Mindfulness-based intervention in context: past, present and future. Clincal Psychology: Sci Pract. 2003; 10(2).
Greeson JM. Mindfulness Research Update: 2008. Complement Health Pract Rev. 2009;14(1):10–8.
Article PubMed PubMed Central Google Scholar
Baer RA. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin Psychol Sci Pract. 2003;10:351–66.
Brown KW, Ryan RM, Creswell JD, Mindfulness. Theoretical foundations and evidence for its salutary effects. Psychol Inq. 2007;18:1–26.
Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits: a meta-analysis. J Psychosom Res. 2004;57:35–43.
Article PubMed Google Scholar
Hoffman S, Sawyer A, Witt A, Oh D. The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. J Consult Clin Psychol. 2010;78(2):169–83.
Vollestad J, Nielsen MB, Nielsen GH. Mindfulness and acceptance-bases interventions for anxiety disorders: a systematic review and meta-analysis. Br J Clin Psychol. 2012;51:239–60.
Ding F, Wu J, Zhang Y. Can mindfulness-based stress reduction relieve depressive symptoms? A systematic review and meta-analysis. J Pac Rim Psychol. 2023;17:1–16.
Nandarathana RJ. The Efficacy and Durability of Mindfulness-based Cognitive Therapy in the Treatment of Anxiety and Depressive Disorders: A Systematic Review and Meta-analysis. Indian Journal of Psychological Medicine. 2024 April; XX: pp. 1-9.
Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Personal Soc Psychol. 2003;84:822–48.
Karremans J, Kappen G, Schellekens M, Schoebi D. Comparing the effects of a mindfulness versus relaxation intervention on romantik relationship wellbeing. Sci Rep. 2020 December;10(1):1–10.
Wachs K, Cordova JV. Mindful relating: exploring mindfulness and emotion repertoires in intimate relationships. J Marital Fam Ther. 2007;33(4):464–81.
Davidson R, Kabat-Zinn J, Schumacher J, Melissa M, Rosenkranz B, Muller D, et al. Alterations in Brain and Immune function produced bya mindfulness meditation. Psychosom Med. 2003;65:564–70.
Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008; 12(4).
Hözel B, Carmody J, Vangel M, Congleton C, Yerramsetti S, Gard T, et al. Mindfulness practice leads to increase in regional brain gray matter density. Psychiatry Research: Neuroimaging. 2011;191:36–43.
Brown KW, Weinstein N, Creswell JD. Trait mindfulness modulates neuroendocrine and affective responses to social evaluative threat. Psychoneuroendocrinology. 2012;37(12):2037–41.
Flook L, Goldberg S, Pinger L, Davidson R. Promoting prosocial behavior and self-regulatory skills in preschool children through a mindfulness-based kindness curriculum. Dev Psychol. 2015; 51(1).
Taylor RD, Oberle E, Durlak JA, Weissberg RP. Promoting positive Youth Development through School-based Social and Emotional Learning interventions: a Meta-Analysis of Follow-Up effects. Child Dev. 2017;88(4):1156–71.
Fabbro A, Crescentini C, Capurso V, D’Antoni F, Crescentini C. Effects of Mindfulness Training on School teachers’ self-reported personality traits as well as stress and burnout levels. Percept Mot Skills. 2020;127(3):515–32.
Blair C. School readiness. Integrating cognition and emotion in a neurobiological conceptualization of children’s functioning at school entry. Am Psychol. 2002;57:111–27.
Moffitt TE, Arseneault L, Belsky D, Dickson N, Hancox RJ, Harrington H, et al. A gradient of childhood self-control predicts health, wealth, and public safety. PNAS. 2011 January;108(7):2693–8.
Zenner C, Herrnleben-Kurz S, Walach H. Mindfulness-based interventions in schools- A systematic review and Meta-analysis. Front Psychol. 2014; 5.
Hwang YS, Bartlett B, Greben M, Hand K. A systematic review of mindfulness interventions for in-service teachers: a tool to enhance teacher wellbeing and performance. Teach Teacher Educ. 2017 February;64:26–42.
Hidajat TJ, Edwards EJ, Wood R, Campbell M. Mindfulness-based interventions for stress and burnout in teachers: A systematic review. Teaching and Teacher Education. 2023 November; 134.
Wood L, Roach AT, Kearney MA, Zabek F. Enhancing executive function skills in preschoolers through a mindfulness-based intervention: a randomized, controlled pilot study. Psychol Sch. 2018;55(6):644–60.
Zelazo PD, Forston JL, Masten AS, Carlson SM. Mindfulness Plus Reflection Training: effects of executive function in early childhood. Front Psychol. 2018; 9.
Lertladaluck K, Suppalarkbunlue W, Moriguchi Y, Chutabhakdikul N. School-based Mindfulness Intervention Improves Executive Functions and self-regulation in preschoolers at risk. J Behav Sci. 2021; 16(2).
Poehlmann-Tynan J, Vigna AB, Weymouth LA, Gerstein ED, Burnson C, Zabransky M, et al. A pilot study of contemplative practices with economically disadvantaged preschoolers: children’s empathic and Self-Regulatory behaviors. Mindfulness. 2015;7:46–58.
Lertladaluck K, Supplarkbunlue W, Moriguchi Y, Chutabhakdikul N. School-based Mindfulness Intervention Improves Executive Functions and self-regulation in preschoolers at risk. J Behav Sci. 2021;16(2):58–72.
Thierry KL, Vincent RL, Bryant HL, Kinder MB, Wise CL. A self-oriented mindfulness-based curriculum improves prekindergarten students’ executive functions. Mindfulness. 2018;9(5):1443–56.
Viglas M, Perlman M. Effects of a mindfulness-based Program on Young Children’s Self-Regulation, Prosocial Behavior and hyperactivity. J Child Fam stud. 2017;27:1150–61.
Kim E, Jackman M, Jo SH, Oh J, Ko SY, McPherson CL, et al. Effectiveness of the mindfulness-based OpenMind-Korea (OM-K) Preschool Program. Mindfulness. 2020 February;11:1062–72.
Razza R, Bergen-Cico D, Raymond K. Enhancing preschoolers’ Self-Regulation Via mindful yoga. J Child Fam stud. 2015;24(2):372–85.
Jackman MM, Nabors LA, McPherson CL, Quaid JD, Singh NN. Feasibility, acceptability, and preliminary effectiveness of the OpenMind (OM) program for Pre-school Children. J Child Fam stud. 2019;28(10):2910–21.
DiCarlo C, Meaux AB, LaBiche EH. Exploring mindfulness for Perceived teacher stress and Classroom Climate. Early Childhood Educ J. 2020 December;48:485–96.
Jennings PA, Doyle S, Oh Y, Rasheed D, Frank JL, Brown JL. Long-term impacts of the CARE program on teachers’ self-reported social and emotional competence and well-being. J Sch Psychol. 2019 October;76:186–202.
Cheng X, Zhang H, Cao J, Ma Y. The Effect of Mindfulness-based programs on psychological distress and burnout in Kindergarten teachers: a pilot study. Early Childhood Educ J. 2022 August;50:1197–207.
Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13:27–45.
Cardaciotto L, Herbert JD, Forman EM, Moitra E, Farrow V. The assessment of present-moment awareness and acceptance. Phila Mindfulness Scale Asessment. 2008;15:204–23.
Feldman G, Hayes A, Kumar S, Greeson J, Laurenceau JP. Mindfulness and emotion regulation: the development and initial validation of cognitive and affective mindfulness scale-revised. J Psychopathol Behav Assess. 2007;29:177–90.
Ma Y. Attachment security, mindfulness, psychotherapy: Testing a mediational model. Doctoral Dissertation. College Park: University of Maryland, Psychology; 2008.
Walach H, Buchheld N, Buttenmuller V, Kleinknecht N, Schmidt S. Measuring mindfulness- the Freiburg Mindfulness Inventory. Pers Indiv Differ. 2006;40:1543–55.
Baer RA, Smith GT, Lykins E, Button D, Krietemeyer J, Sauer S, et al. Construct validity of the five-facet mindfulness questionnaire in meditating and non-meditating samples. Assessment. 2008;15:329–42.
Becker B, Gallagher K, Whitaker R. Teachers’ dispositional mindfulness and the quality of their relationships with children in Head Start classrooms. J Sch Psychol. 2017;65:40–53.
Anama-Green C. Intrapersonal mindfulness is associated with reduced risk of burnout among Central Appalachian educators. Explore. 2022;18(1):64–49.
Solari B. Pre-validación del cuestionario five-facet mindfulness questionnaire. Tesis de Magister. Santiago: Pontificia Universidad Católica de Chile, Escuela de Psicología; 2010.
Lovibond S, Lovibond P. Manual for the depression anxiety stress scales Sydney. Psychology Foundation of Australia; 1995.
Antúnez Z, Vinet EV. Escalas De Depresión, Ansiedad Y Estrés (DASS-21): Validación De La versión abreviada en estudiantes universitarios chilenos. Terapia Psicológica. 2012;30(3):49–55.
Román F, Vinet E, Alarcón AM. Escalas De Depresión, Ansiedad Y Estrés (DASS-21): Adaptación Y propiedades psicométricas en estudiantes secundarios de Temuco. Revista Argentina De Clínica Psicológica. 2014;23(2):179–90.
Maslach C, Jackson S. Stress, burnout, and workaholism. In: Kilburg RR, Nathan PE, Thoreson RW, editors. Professionals in distress: issues, syndromes, and solutions in psychology. American Psychological Association; 1981. pp. 53–75.
O’Rourke HP, MacKinnon DP. Reasons for testing mediation in the absence of an intervention effect: a Research Imperative in the Prevention and Intervention Research. J Stud Alcohol Drugs. 2018;79(2):171–81.
Valeri L, VanderWeele TJ. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: theoretical assumptions and implementation with SAS and SPSS macros. Psychol Methods. 2013;18(2):137.
Cash M, Whittingham K. What facets of mindfulness contribute to psychological well-being and depressive, anxious and stress-related symptomatology? Mindfulness. 2010;1:177–82.
Corthorn C, Milicic N. Mindfulness and parenting: a correlational study of non-meditating mothers of preschool children. J Child Fam stud. 2016;25(5):1672–83.
Ortet G, Pinazo D, Walker D, Gallego S, Mezquita L, Ibañez MI. Personality and nonjudging make you happier: contribution of the five-factor model, mindfulness facets and a mindfulness intervention to subjective well-being. PLoS ONE. 2020; 15(2).
Diehl J, Rodriguez-Seijas C, Thompson J, Dalrymple K, Chelminski I, Zimmerman M. Exploring the Optimas factor structure of the five Facet Mindfulness Questionnaire: associations between Mindfulness facets and dimensions of psychopathology. J Pers Assess. 2022;104(6):813–23.
Fritz MS, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–9.
Caron PO. A comparison of the type I error rates of three assessment methods for indirect effects. J Stat Comput Simul. 2019;89(8):1343–56.
Gunasekaran K, Vasudevan K, Srimadhi M. Assessment of mental health status among adolescents in Puducherry, India - A mixed method study. Journal of Family Medicine and Primary Care. 2022 Junio; 11.
Paz-Soto P, Games-Díaz L, Ramírez-Santana M. Characterization of suicidal behavior in Coquimbo, Chile, between 2018 and 2020. Medwave. 2024; 24(2).
Download references
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Universidad Andres Bello’s Internal Projects Funding “Nucleo 2021” [N° DI-03-21/NUC].
Author information
Authors and affiliations.
Department of Education and Social Sciences, Facultad de Educación, Universidad Andrés Bello, Fernández Concha 700, Edificio C2, Tercer Piso, Las Condes, Santiago, Chile
Carolina Corthorn & Natalia Torres
Faculty of Nursing, Universidad Andrés Bello, Santiago, Chile
Víctor Pedrero & Katiuska Reynaldos-Grandón
Department of Social Sciences, Universidad Central de Chile, Santiago, Chile
Paola Paredes
You can also search for this author in PubMed Google Scholar
Contributions
The authors confirm contributions to the paper as follows: study conception and design: C.C., V. P, N.T., K.R., P.P.; data collection: C.C, N.T, P.P.; analysis and interpretation of results: C.C., V.P.; draft manuscript preparation: C.C., V. P. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Correspondence to Carolina Corthorn .
Ethics declarations
Ethics approval and consent to participate.
All procedures performed in this study were approved by the bioethical committee of the Universidad Andres Bello and in accordance with the 1964 Helsinki declaration and its later amendments. Informed consent for participation and for the use of the results for research purposes was obtained individually from all the participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Corthorn, C., Pedrero, V., Torres, N. et al. Mindfulness, teacher mental health, and well-being in early education: a correlational study. BMC Psychol 12 , 428 (2024). https://doi.org/10.1186/s40359-024-01930-3
Download citation
Received : 17 July 2023
Accepted : 29 July 2024
Published : 06 August 2024
DOI : https://doi.org/10.1186/s40359-024-01930-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Mindfulness
- Mental health
- Quality of life
- Preschool teachers
BMC Psychology
ISSN: 2050-7283
- General enquiries: [email protected]
Watch CBS News
Excessive smartphone use can negatively impact teen's mental health, researchers find
By Mallika Marshall, MD
Updated on: August 5, 2024 / 5:48 PM EDT / CBS Boston
BOSTON - Researchers have found more evidence that excessive smartphone use could impact a teen's mental health.
Scientists refer to it as "problematic smartphone use" or PSU; in other words, behaviors around smartphone use akin to an addiction, including an inability to limit the amount of time spent on the phone, feeling panicky when the phone is out of reach, or using it when they should be doing other activities.
Researchers at King's College London found that teens with PSU were twice as likely to have anxiety and almost three times more likely to suffer from depression compared to teens without problematic smartphone use.
Older teens also reported higher rates of insomnia. Most kids said they wanted to cut down on their phone use, and some said they needed help to do it. Some strategies that work include putting the phone in silent mode, getting rid of notifications, and placing the phone in another room at bedtime.

Mallika Marshall, MD is an Emmy-award-winning journalist and physician who has served as the HealthWatch Reporter for CBS Boston/WBZ-TV for over 20 years. A practicing physician Board Certified in both Internal Medicine and Pediatrics, Dr. Marshall serves on staff at Harvard Medical School and practices at Massachusetts General Hospital at the MGH Chelsea Urgent Care and the MGH Revere Health Center, where she is currently working on the frontlines caring for patients with COVID-19. She is also a host and contributing editor for Harvard Health Publications (HHP), the publishing division of Harvard Medical School.
Featured Local Savings
More from cbs news.

Health department shuts down Norwood boy's charity ice cream stand after complaint

Steward Health Care selling doctors network to group owned by private equity firm

The best state to live in is Massachusetts, new ranking says

Restaurant donates part of dessert sales to boy whose ice cream stand was shut down

Moms think more about household chores − and this cognitive burden hurts their mental health

Professor of Psychology, USC Dornsife College of Letters, Arts and Sciences

Ph.D. Candidate in Psychology, University of Southern California
Disclosure statement
Darby Saxbe receives funding from NIH, NSF, and Hello Sunshine, the company which licenses the Fair Play system for the division of household labor.
Lizzie Aviv receives funding from and consults for Hello Sunshine, the company that licenses the Fair Play system.
USC Dornsife College of Letters, Arts and Sciences and University of Southern California provide funding as members of The Conversation US.
View all partners
When you think about housework, you likely think of actions: scrubbing the dishes, running errands, chopping vegetables for dinner. And it’s not news to say that mothers often shoulder the burden for most of those activities.
But there’s an invisible dimension of household labor that unfolds behind the scenes: the cognitive effort that goes into anticipating needs, planning, organizing and delegating household tasks. In other words, someone has to remember to replace the dish soap and select which vegetables to chop.
Our new research found that this cognitive dimension of housework, often called the “mental load,” is divided even more unevenly within couples than the physical dimension – and it seems to take a particular mental health toll on women. According to the study we published in the Archives of Women’s Mental Health, mothers who take on a more disproportionate share of cognitive household labor report higher levels of depression, stress, relationship dissatisfaction and burnout.
Tracking who does what
We asked 322 mothers of young children about who in their family is responsible for 30 common household tasks. We collaborated with the creators of the Fair Play system – a book and card game designed to better quantify the division of labor within households – to divide each task into two dimensions: cognitive (anticipating, planning, delegating and thinking about household tasks) and physical (the hands-on execution of household tasks). We then examined how these tasks are shared between partners.
We found a striking gender disparity: Mothers not only performed more physical housework but also carried a significantly greater share of cognitive labor compared with their partners.
On average, mothers reported being responsible for about 73% of all cognitive household labor compared with their partners’ 27%, and 64% of all physical household labor compared with their partners’ 36%. Indeed, for every single task we examined, the gender difference was larger for the cognitive dimension than the physical execution dimension.
There was only one task in which fathers did more planning and execution: taking out the garbage. Fathers also carried out more home maintenance tasks, but mothers did more of the related planning.
Interestingly, while an unequal division of physical tasks was linked to worse couple relationship quality, it was the cognitive labor that had a more profound impact on women’s psychological well-being.
Family dynamics have societal impact
An unequal division of household labor is a key driver of global gender inequity , suppressing women’s full participation in the paid workforce and significantly affecting women’s health and well-being .
Our study is one of the first to investigate the cognitive dimension of household labor and its effects on maternal mental health. Cognitive labor may be particularly taxing for women because it often runs behind the scenes and goes unacknowledged or unappreciated by others . It also pulls mental energy away from other priorities.
Additional studies indicate that women experience more negative effects from child care and housework compared with men, such as higher depression rates, partly due to the heavier cognitive load they carry.

What still isn’t known
Our study was limited by its reliance on self-reported household labor and by the fact that we were able to collect data only from mothers in cohabiting, heterosexual couple relationships. Future studies can survey both partners and directly observe what chores couples do at home. They can also look at different kinds of relationship configurations, including gay and lesbian couples.
We also don’t know much about the long-term effects of the division of cognitive labor on women’s mental health and cognitive functioning.
The unfair division of housework is a frequent source of stress in relationships and often cited by women as a reason for divorce . The cognitive load may be an underappreciated aspect of the domestic workload that warrants more attention from couples therapists, mental health counselors and premarital relationship educators.
- Gender inequality
- Gender equality
- Household chores
- Household work
- Division of labor
- Gender disparities
Want to write?
Write an article and join a growing community of more than 188,200 academics and researchers from 5,015 institutions.
Register now
mental health center / mental health a-z list / how excessive heat can affect your mental health article
- How Excessive Heat Can Affect Your Mental Health
Latest Mental Health News
- Obamacare Boosted New Mom Access to Mental Health
- Brain Study Shows How Classical Music Lifts Mood
- TikTok Glamorize Eating Disorders Harm Body Image
- How Likely Is It That Autism Recurs in One Family

As Americans sweat through another scorching summer, one expert warns that while extreme heat can cause physical harm it can also wreak havoc with your mental health .
Sizzling temperatures can make anyone irritable, but it can be far worse for some, especially those with mental health conditions, said Dr. Asim Shah, executive vice chair in the Menninger Department of Psychiatry and Behavioral Sciences at Baylor College of Medicine in Houston. Excessive heat can trigger feelings of anger, irritability, aggression, discomfort, stress and fatigue because of its impact on serotonin, the neurotransmitter that regulates your sleep , mood and behaviors, Shah noted. The most vulnerable groups include people with preexisting mental health conditions and people who abuse alcohol or other drugs . “All mental illnesses increase with heat because it results in more fatigue , irritability and anxiety , and it can exacerbate depressive episodes ,” Shah explained in a Baylor news release. What are the signs of impending trouble? They tend to start with irritability, decreased motivation, aggressive behavior and sometimes mental fogging. In worse cases, confusion and disorientation occur, Shah noted.
While avoiding the heat may not be possible, Shah recommends hydrating and keeping your head covered when going outside. If it gets too hot, pour some water on your head to cool down and try doing things in the shade. If you normally go for walks outside, try walking in the mall or a large space with air conditioning. If you take medications, consult with your provider because some medications for mental health, such as lithium for bipolar patients, don't pair well with heat. Lithium goes through the kidney, so sweating can have an impact on the levels of the medication in your body, Shah explained. “If you are out in the heat and using lithium, levels may fluctuate. In that scenario, we have to be very careful and either adjust the dosage of lithium or avoid heat,” he noted. Droughts and extreme changes in temperature can also increase levels of pollutants and allergens as air quality worsens. That can exacerbate mental health issues like depression , anxiety or PTSD . Some studies show that exposure to any natural climate disaster can raise the risk of depression by more than 30%, anxiety by 70% and both by over 87%, Shah said.
Kids are not immune to the effects of intense heat, either. “Children are a vulnerable population due to their physical and cognitive immaturity. They are exposed to more pollutants and allergens as they spend more time outdoors,” Shah noted. If you feel affected by severe heat, call your doctor or mental health specialist.
SOURCE: Baylor College of Medicine, news release, July 24, 2024

Related Article

What's Your Biggest Fear? Phobias
Learn about phobias such as agoraphobia, claustrophobia, arachnophobia, zoophobia, and more. Discover some of the symptoms and treatments of phobias.
Read more: What's Your Biggest Fear? Phobias
Transforming the understanding and treatment of mental illnesses.
Información en español
Celebrating 75 Years! Learn More >>
- Research Funded by NIMH
- Research Conducted at NIMH (Intramural Research Program)
- Priority Research Areas
- Research Resources
How Emotional States affect Decision-Making
Join a Research Study: Enrolling locally from the Washington, D.C. metro region
To find out if you qualify, email the study team ([email protected] ) or call (301) 451-7822 [TTY: 711].
How we feel can impact the choices we make. Feelings of sadness, stress, or pain can change our behavior. Researchers want to learn more about the choices we make when feeling bad. By learning more about how emotions affect thinking and behavior, we hope to better understand how to identify and treat people with mental disorders.
You may be able to participate in this outpatient study if you are:
- Ages 18-55 years old
- Do not have a diagnosed mental health condition
- Are otherwise medically healthy
Participation includes a medical evaluation, questionnaires, and a situation to cause a temporary change in emotional state (unpleasant physical/emotional feeling such as from mild pain, snack craving, or stress.)
This study includes 3 visits to the NIH Clinical Center in Bethesda, MD. Compensation is provided.
Study Identifiers
- NIMH Protocol Number: 000978-M
- ClinicalTrials.gov Study Number: 05666726
Investigator(s): Silvia Lopez-Guzman, M.D., Ph.D.
- Share full article
Advertisement
Supported by
Idaho Murders Suspect Felt ‘No Emotion’ and ‘Little Remorse’ as a Teen
Messages and online posts from the Ph.D. student now charged with four murders show that he was once detached and suicidal before he became fascinated with criminals’ minds.

By Mike Baker and Nicholas Bogel-Burroughs
MOSCOW, Idaho — A criminology Ph.D. student charged with stabbing four University of Idaho students to death had written years ago of having suicidal thoughts, not being able to feel emotions and observing his own life as if it were a video game, saying he could do “whatever I want with little remorse.”
The new revelations about the suspect, Bryan Kohberger, come from posts he made on an online forum in which he discussed his mental health struggles, as well as from interviews with those who knew him and messages he sent to friends that were obtained by The New York Times.
They paint a portrait of an anxious, isolated and depressed teenager who turned to heroin use before eventually getting clean and becoming fascinated with studying criminal psychology, saying then that he hoped to one day provide counseling for high-profile criminals.
“I feel like an organic sack of meat with no self worth,” he wrote in 2011, when he was 16, adding later, in the same post: “As I hug my family, I look into their faces, I see nothing, it is like I am looking at a video game, but less.”
Now, Mr. Kohberger, 28, is facing murder charges, accused of sneaking into a home shared by students just off the university campus in Moscow, Idaho, and stabbing four of them to death, in the middle of the night. At the time of the killings, Mr. Kohberger was in the first semester of his Ph.D. program at Washington State University, a 15-minute drive from the crime scene.
He has maintained his innocence through his lawyer, and on Thursday waived his right to a speedy preliminary hearing. A judge set a June date for the hearing, when prosecutors will outline evidence in an attempt to prove they have probable cause to try him on murder charges.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
- Search the site GO Please fill out this field.
- Newsletters
- Financial Health
How Debt Affects Mental Health—And What Can You Do About It
:max_bytes(150000):strip_icc():format(webp)/IMG_3667-MikaylaMorell-b16b23a635e248fcbbad3d1ae1a702fa.JPG "homework mental health affect")
Why Is Debt Linked to Suicide?
- Impact on Mental Health
- When to Seek Help
Research has shown that people who experience stress from financial issues and debt are 20 times more likely to attempt suicide than those who do not experience this type of stress. What's more, financial hardship is, unfortunately, a common problem. In one study, over 50% of the participants reported having two or more financial stressors.
A report noted that the average American is $52,940 in debt. This debt includes:
- Credit card debt
- Medical bills
- Money owed for mortgages and leases
- Personal loans
- Student loan debt
While many people are keenly aware of how financial stress impacts our lives, it can also have physiologic effects—causing everything from headaches and insomnia to abdominal discomfort. However, most people don't know that financial hardship causes significant mental health distress and is a major risk factor for suicide.
Jordi Salas / Getty Images
Financial hardship makes suicide more likely because worrying about money can cause extreme levels of stress as well as other types of emotional distress. Experiencing a financial crisis, low socioeconomic status, or the strain of bills you can't pay may also negatively impact a person's self-worth or feelings of helplessness, which can make suicide more likely.
What Causes Debt?
Debt happens when your living expenses and other spending exceed your income. If this pattern continues over time, debt can quickly accumulate. Credit card debt and other interest and fees on purchases, mortgages, rent, or other bills can further exacerbate financial hardship—and stress, increasing the risk of suicide.
One study identified a correlation between suicide and four financial stressors:
Homelessness
Unemployment.
The study explored how these stressors play a major role in suicides.
Researchers found that the risk of suicide grew with each added stressor—and those who experienced all four financial stressors were 20 times more likely to attempt suicide.
Homelessness is directly related to financial issues. Mental health conditions are one of the factors that can contribute to homelessness. Homelessness can also contribute to someone developing a mental health condition. Either way, people who experience homelessness often have mental health conditions.
Homelessness can also lead to problems such as:
- Difficulty staying safe
- Limited access to healthcare
- Problems getting food
People who are experiencing unemployment may be experiencing financial difficulties due to a lack of steady income and/or depleting savings. Unemployment can lead to negative mental health effects such as:
- Demoralization
- Low self-esteem
Debt and Low Income
The study found that both financial debt and low income were associated with suicidal ideations and attempts.
Research shows that a person's overall health and well-being can improve if their debt is canceled or reduced. There is also evidence that a higher income is associated with an improvement in health for people of low and moderate income.
Unfortunately, canceling debt and obtaining a higher income isn't easy, but financial education and counseling may help reduce the burden of debt and low income.
How Does Debt Cause Mental Health Issues?
Financial stress is a major risk factor for suicide. Stress, of any kind, can lead to symptoms of depression and anxiety. Having loans and other debt can increase anxiety, distress, and depression levels—all of which can put someone at risk for suicidal ideations.
Unfortunately, mental health conditions and financial stress reinforce one another—people who experience mental health conditions are more likely to experience financial hardship, and financial stress can contribute to mental health problems. Mental health conditions can also make it difficult to recover from financial stress.
It's a loop that can be difficult to get out of—but you have options.
Financial hardship can make people up to 20 times more likely to make an attempt on their lives.
What To Do About Debt and Financial Stress
If you are struggling with debt, homelessness, unemployment, and/or feelings of hopelessness, know that you are not alone—there is both help and hope.
Places to find assistance include local social services offices, credit counseling services, credit unions, community organizations, friends, relatives, and banks.
Reaching out is not a sign of weakness and does not mean you have failed as a provider, parent, or spouse. Rather, it means that you can recognize that your financial situation is putting you under stress and you want to address it.
It's important to take a multifaceted approach that addresses the financial stressors and their impact on your mental health.
Seek Mental Health Counseling
The first step is getting help. Talking to a mental healthcare provider about the thoughts or anxiety symptoms you may be experiencing may be helpful in dealing with financial stress.
If it feels like an overwhelming catastrophe, you can work through and process this with a trained mental health clinician who can help you learn ways to reduce those overwhelming thoughts.
Speaking to someone you trust can help you ease the weight of it, gain insight into ways to manage it, and create a plan.
Seek Financial Counseling
You may consider calling a financial advisor or counselor to strategize potential solutions or options. You can find free or low-cost counseling services at places like:
- Credit unions
- Extension offices
- Nonprofit agencies
- Religious organizations
- Universities
When you see a counselor, they will discuss your finances and help you create a personalized plan and budget. They can also help you find programs on money management.
Even if you have a friend or loved one to talk to for emotional support, it is always a good idea to take practical advice from an expert.
Learn How To Budget
A financial counselor can help you learn how to budget, but if you want to try it on your own, it's an important skill to have in order to manage your money.
The easier it becomes to manage your money, the less stress you'll take on. Here are the basic steps for making a budget:
- Write down your expenses.
- Write down your income (how much money you make).
- Subtract your expenses from your income.
- If the amount is less than zero, it will likely be necessary to try to make some changes to your spending.
- Look at your budget and see where you spend your money, where you could spend less, and what you want to contribute more money to (housing, savings, debt, etc.)
The information in your budget can help you better prepare for your expenses.
When To Seek Emergency Help for Debt or Suicide Ideation
If you or someone you know is having suicidal thoughts due to stress of debt or monetary hardship, seek emergency help—call 988 (the suicide hotline), 911, or get to your nearest emergency department. Also, call someone you trust—a friend, family member, co-worker, or clergy person.
Looking for support?
If you or someone you know is in crisis, call the National Suicide Prevention Lifeline at 988 or 1-800-273-TALK (8255) or contact the Crisis Text Line by texting TALK to 741-741.
A Quick Review
Financial hardship is a common issue in the United States. Financial stresses—including homelessness, unemployment, debt, and low income—can have a negative impact on a person's mental health, leading to anxiety, depression, and other mental health conditions.
Mental health conditions can put someone at risk for suicidal thoughts and attempts. If you or someone you know is struggling with finances, you can seek help through a mental health counselor and a financial counselor, or you can call the National Suicide Prevention Lifeline at 988 for immediate support.
Elbogen EB, Lanier M, Montgomery AE, Strickland S, Wagner HR, Tsai J. Financial strain and suicide attempts in a nationally representative sample of us adults . American Journal of Epidemiology . 2020;189(11):1266-1274. doi:10.1093/aje/kwaa146
Weissman J, Russell D, Mann JJ. Sociodemographic characteristics, financial worries and serious psychological distress in U.S. adults . Community Ment Health J . 2020;56(4):606-613. doi:10.1007/s10597-019-00519-0
Federal Reserve Bank of New York. Center for microeconomic data .
Anxiety & Depression Association of America. How to calm an anxious stomach: the brain-gut connection .
MedlinePlus. Migraine .
Centers for Disease Control and Prevention. Risk and protective factors .
Ryu S, Fan L. The Relationship Between Financial Worries and Psychological Distress Among U.S. Adults . J Fam Econ Issues . 2023;44(1):16-33. doi:10.1007/s10834-022-09820-9
Rojas Y. Financial indebtedness and suicide: A 1-year follow-up study of a population registered at the Swedish Enforcement Authority . Int J Soc Psychiatry . 2022;68(7):1445-1453. doi:10.1177/00207640211036166
García de la Garza Á, Blanco C, Olfson M, Wall MM. Identification of suicide attempt risk factors in a national us survey using machine learning . JAMA Psychiatry . 2021;78(4):398. doi:10.1001/jamapsychiatry.2020.4165
Consumer.gov. Making a budget .
MedlinePlus. Homelessness and health .
Office of Disease Prevention and Health Promotion. Employment .
American Public Health Association. The impacts of individual and household debt on health and well-being .
Ryu S, Fan L. The relationship between financial worries and pychological distress among U.S. adults . J Fam Econ Issues . 2023;44(1):16-33. doi:10.1007/s10834-022-09820-9
Federal Trade Commission. How to Get Out of Debt .
Guan N, Guariglia A, Moore P, Xu F, Al-Janabi H. Financial stress and depression in adults: A systematic review . PLoS One . 2022;17(2):e0264041. doi:10.1371/journal.pone.0264041
USAGov. Facing Financial Hardship .
Related Articles
COMMENTS
Emmy Kang, mental health counselor at Humantold , says studies have shown heavy workloads can be "detrimental" for students and cause a "big impact on their mental, physical and emotional health ...
A Stanford researcher found that too much homework can negatively affect kids, especially their lives away from school, where family, friends and activities matter. "Our findings on the effects ...
Health Hazards of Homework. Pediatrics. A new study by the Stanford Graduate School of Education and colleagues found that students in high-performing schools who did excessive hours of homework "experienced greater behavioral engagement in school but also more academic stress, physical health problems, and lack of balance in their lives.".
Beyond that point, kids don't absorb much useful information, Cooper says. In fact, too much homework can do more harm than good. Researchers have cited drawbacks, including boredom and burnout toward academic material, less time for family and extracurricular activities, lack of sleep and increased stress.
Key points. Mental health challenges and neurodevelopmental differences directly affect children's ability to do homework. Understanding what difficulties are getting in the way—beyond the usual ...
But they also say the answer may not be to eliminate homework altogether. Emmy Kang, mental health counselor at Humantold, says studies have shown heavy workloads can be "detrimental" for students ...
Lack of sleep. One of the most prevalent adverse effects of schoolwork is lack of sleep. The average student only gets about 5 hours of sleep per night since they stay up late to complete their homework, even though the body needs at least 7 hours of sleep every day. Lack of sleep has an impact on both mental and physical health.
Homework — a dreaded word that means more work and less play. The mere thought of doing additional work after a seven-hour day (that begins extremely early) can be gruesome. Not to mention, many ...
Even before the pandemic, U.S. students were struggling with mental health. But the statistics have since become even more alarming. According to a new federal of teen health, about 1 in 5 adolescents report symptoms of anxiety or depression. The impact of social media and bullying have, for good reason, dominated much of the discussion around this growing crisis.
The promotion of mental health among children and adolescents is a public health imperative worldwide, and schools have been proposed as the primary and targeted settings for mental health promotion for students in grades K-12. This review sought to provide a comprehensive understanding of key factors involved in models of school education ...
In a Gallup poll of over 2,400 college students in 2023, 66% of students reported experiencing stress, and 51% stated they experience worry "during a lot of the day."While some levels of stress may be expected, chronic academic stress can significantly harm the mental health of high school and undergraduate university students.
Studies of typical homework loads vary: In one, a Stanford researcher found that more than two hours of homework a night may be counterproductive.The research, conducted among students from 10 high-performing high schools in upper-middle-class California communities, found that too much homework resulted in stress, physical health problems and a general lack of balance.
Introduction. Homework, or between-session practice of skills learned during therapy, is one of the most integral, yet underutilized components of high-quality, evidence-based mental health care (Kazantzis & Deane, 1999).Homework activities (e.g., self-monitoring, relaxation, exposure, parent behavior management) are assigned by providers in-session and completed by patients between sessions ...
There is a non-linear relationship between homework time and adolescent mental health. Homework negatively impacts adolescent mental health, but only when exceeding about 1 h and 15 min. Teacher support, particularly emotional support, can mitigate the adverse mental health effects of excessive homework time. Abstract.
Emmy Kang, mental health counselor at Humantold, says studies have shown heavy workloads can be "detrimental" for students and cause a "big impact on their mental, physical and emotional health ...
The mental effects of homework can be harmful as well. Mental health issues are often ignored, even when schools can be the root of the problem. An article from USA Today contained a quote from a licensed therapist and social worker named Cynthia Catchings, which reads, " heavy workloads can also cause serious mental health problems in the ...
This increase in education had an effect on mental health more than 2 decades later. An extra year of education led to a lower likelihood of reporting any symptoms related to depression (11.3%) and anxiety (9.8%). More educated people also suffered less severe symptoms - depression (6.1%) and anxiety (5.6%).
Pope and her colleagues found that too much homework can diminish its effectiveness and even be counterproductive. They cite prior research indicating that homework benefits plateau at about two hours per night, and that 90 minutes to two and a half hours is optimal for high school. • Greater stress: 56 percent of the students considered ...
A 2013 study conducted at Stanford University found that students in top-performing school districts who spend too much time on homework experience more stress, physical health problems, a lack of balance in their lives and alienation from society.
5. Homework and Mental health statistics. The findings on homework relation to mental health were so troubling since the report showed that too many homework tasks are associated with high levels of stress, physical health condition, and lack of balance in students' lives. Fifty-seven percent of the children in the research cited that ...
That can exacerbate mental health issues like depression, anxiety or PTSD. Some studies show that exposure to any natural climate disaster can raise the risk of depression by more than 30% ...
President George H. W. Bush proclaimed the 1990s "The Decade of the Brain ," urging the National Institutes of Health, the National Institute of Mental Health (NIMH), and others to raise awareness about the benefits of brain research. "Over the years, our understanding of the brain—how it works, what goes wrong when it is injured or diseased—has increased dramatically.
Work stress not only affects the physical and mental health of the teacher, but symptoms of burnout, such as irritability, discouragement and hyperreactivity to stress, represent serious interference in the teacher-student relationship and therefore affect the effectiveness of the teaching-learning process [].An unmotivated and irritated teacher who is working with great emotional distance ...
Excessive phone usage can affect a teenager's mental health, research shows 01:03. BOSTON - Researchers have found more evidence that excessive smartphone use could impact a teen's mental health.
According to the study we published in the Archives of Women's Mental Health, mothers who take on a more disproportionate share of cognitive household labor report higher levels of depression, ...
The most vulnerable groups include people with preexisting mental health conditions and people who abuse alcohol or other drugs. "All mental illnesses increase with heat because it results in more fatigue, irritability and anxiety, and it can exacerbate depressive episodes," Shah explained in a Baylor news release.
By learning more about how emotions affect thinking and behavior, we hope to better understand how to identify and treat people with mental disorders. You may be able to participate in this outpatient study if you are: Ages 18-55 years old; Do not have a diagnosed mental health condition; Are otherwise medically healthy
Jan. 13, 2023. MOSCOW, Idaho — A criminology Ph.D. student charged with stabbing four University of Idaho students to death had written years ago of having suicidal thoughts, not being able to ...
Connecting dental and mental health One of the first studies to document the link between gum disease, tooth loss and Alzheimer's disease focused on a cohort of aging nuns who were part of a ...
Elbogen EB, Lanier M, Montgomery AE, Strickland S, Wagner HR, Tsai J. Financial strain and suicide attempts in a nationally representative sample of us adults. American Journal of Epidemiology ...